Canine hypothyroidism is considered a classic endocrinopathy with characteristic clinical manifestations. Despite seemingly clear clinical symptoms, establishing an accurate diagnosis remains a significant challenge.
Numerous retrospective studies have shown that up to 70% of dogs treated with levothyroxine (L-thyroxine) do not actually have hypothyroidism. The substantial discrepancy between the reported diagnostic rate and the true prevalence (estimated at 0.07–0.23%) highlights the need for a more refined diagnostic approach.
Non-thyroidal illness (NTI), the effects of medications, and method-related misinterpretations further complicate the diagnostic process.
Indiscriminate initiation of levothyroxine therapy carries the risk of overlooking relevant underlying conditions and unnecessarily increasing the metabolic stress. In the presence of concurrent heart disease or untreated/unrecognised hypoadrenocorticism, this can lead to decompensation and may be potentially fatal.
In this diagnostic grey zone, novel approaches such as the measurement of reverse T3 (rT3) and the analysis of relevant parameters using liquid chromatography–tandem mass spectrometry (LC-MS/MS) provide valuable additional diagnostic options.
Basics of Thyroid Physiology and Diagnostics
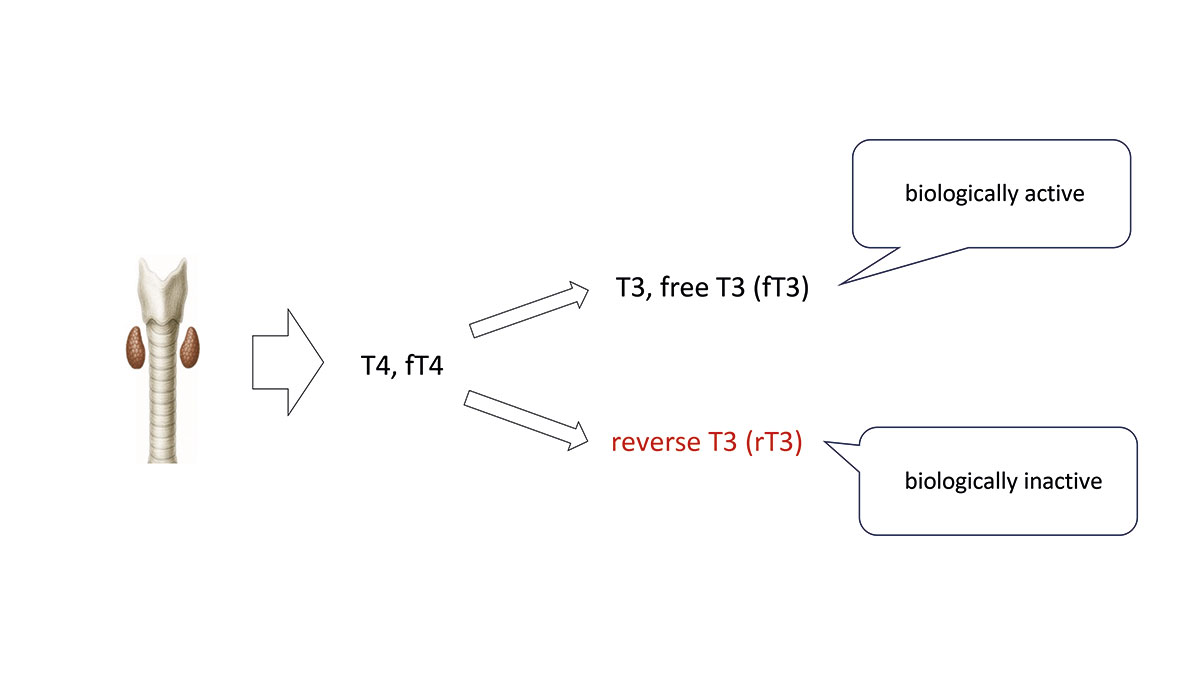
Thyroid function is regulated by the complex interaction within the hypothalamic-pituitary-thyroid axis. TRH released from the hypothalamus stimulates TSH secretion in the pituitary gland, which in turn triggers the thyroid gland to synthesise and secrete thyroid hormones, primarily thyroxine (T4). In serum, more than 99% of T4 is protein-bound, with total T4 comprising both the protein-bound and free fractions. Only the free fraction (fT4) is taken up into cells, where it undergoes 5′-deiodination being metabolized to triiodothyronine (T3), the biologically active hormone at the cellular level.
Alternatively, fT4 can be converted into biologically inactive reverse T3 (rT3), which is thought to play a role in cellular regulation and in preventing excessive levels of active T3.
-

-
Fig. 1: Schematic representation of fT4 metabolism within the target cell into T3 and rT3
Image source: J. von Luckner
-
-
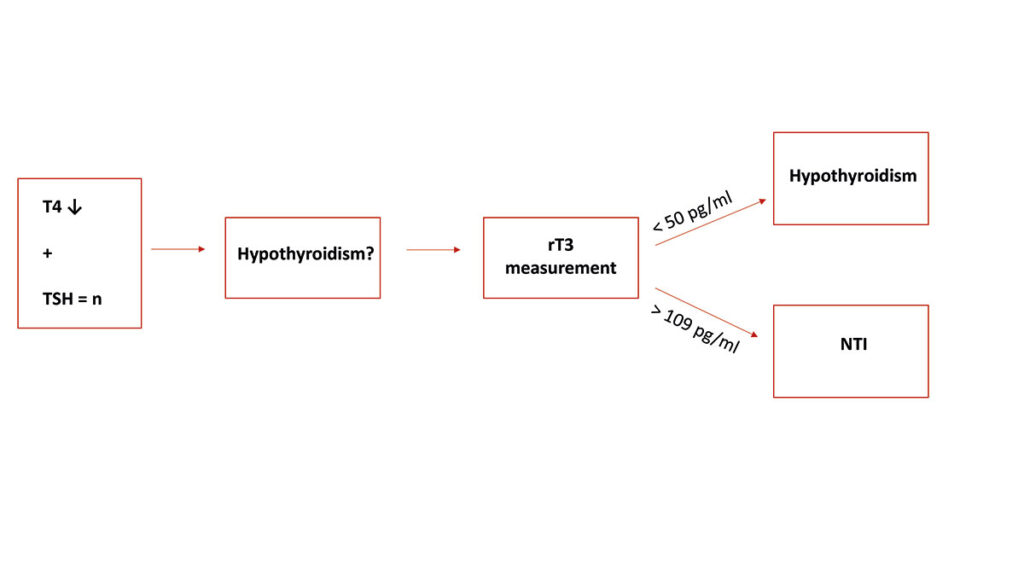
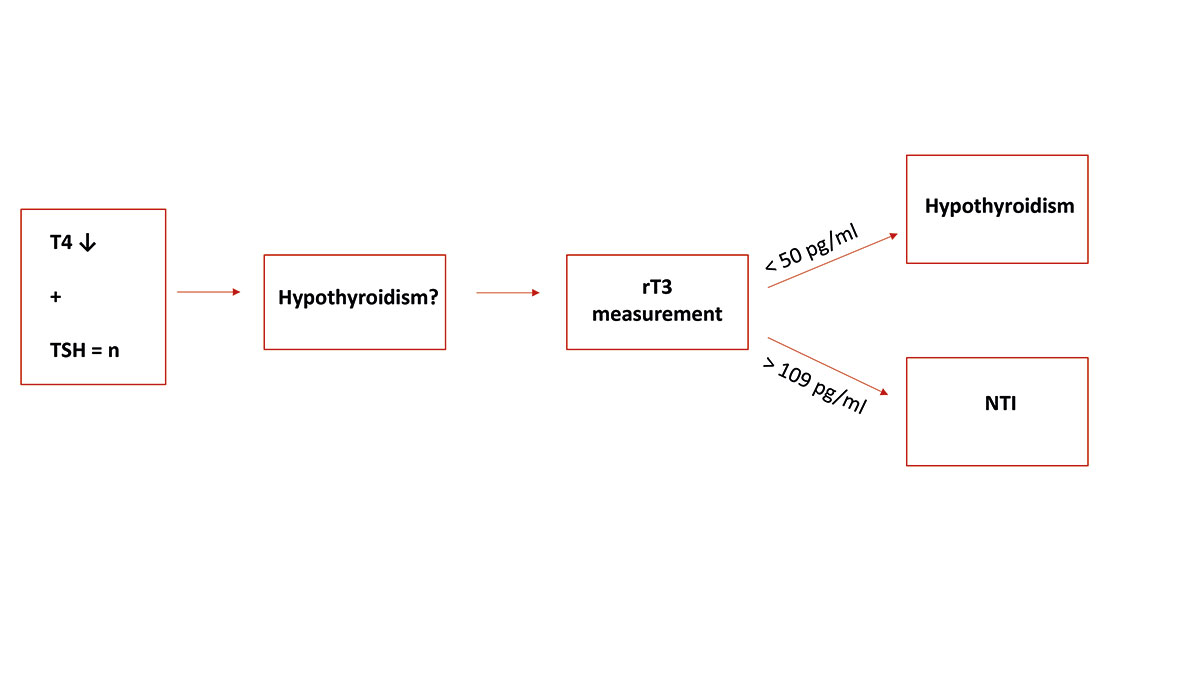
Fig. 2: Diagnostic guide for rT3
Image source: Niklas Wiesner
-
-
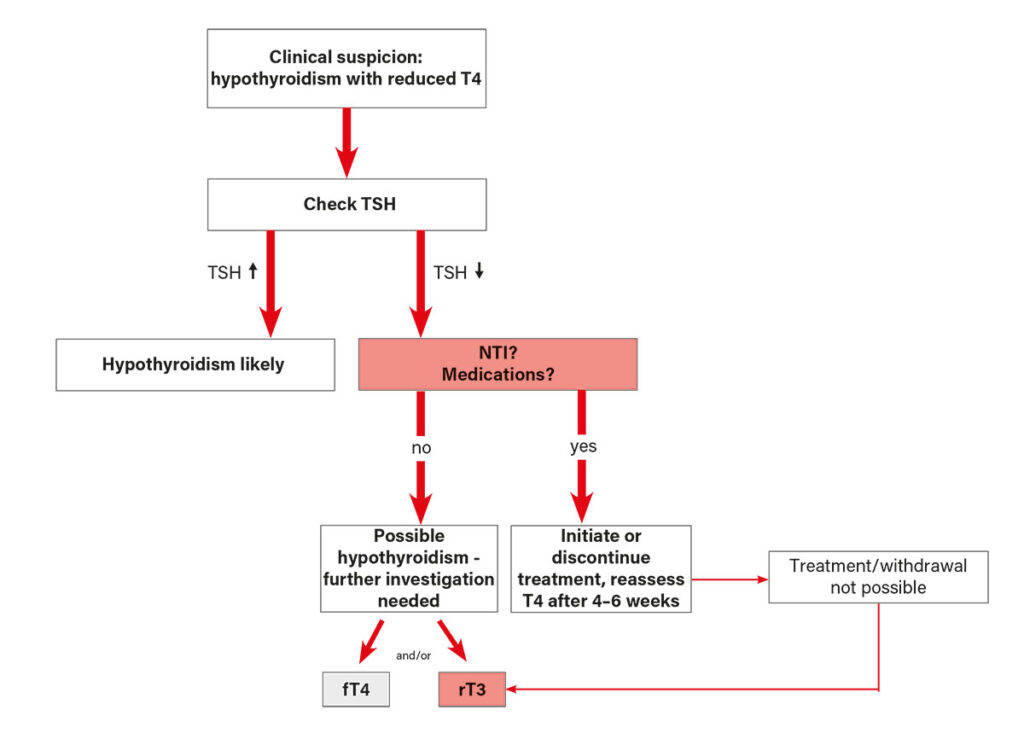
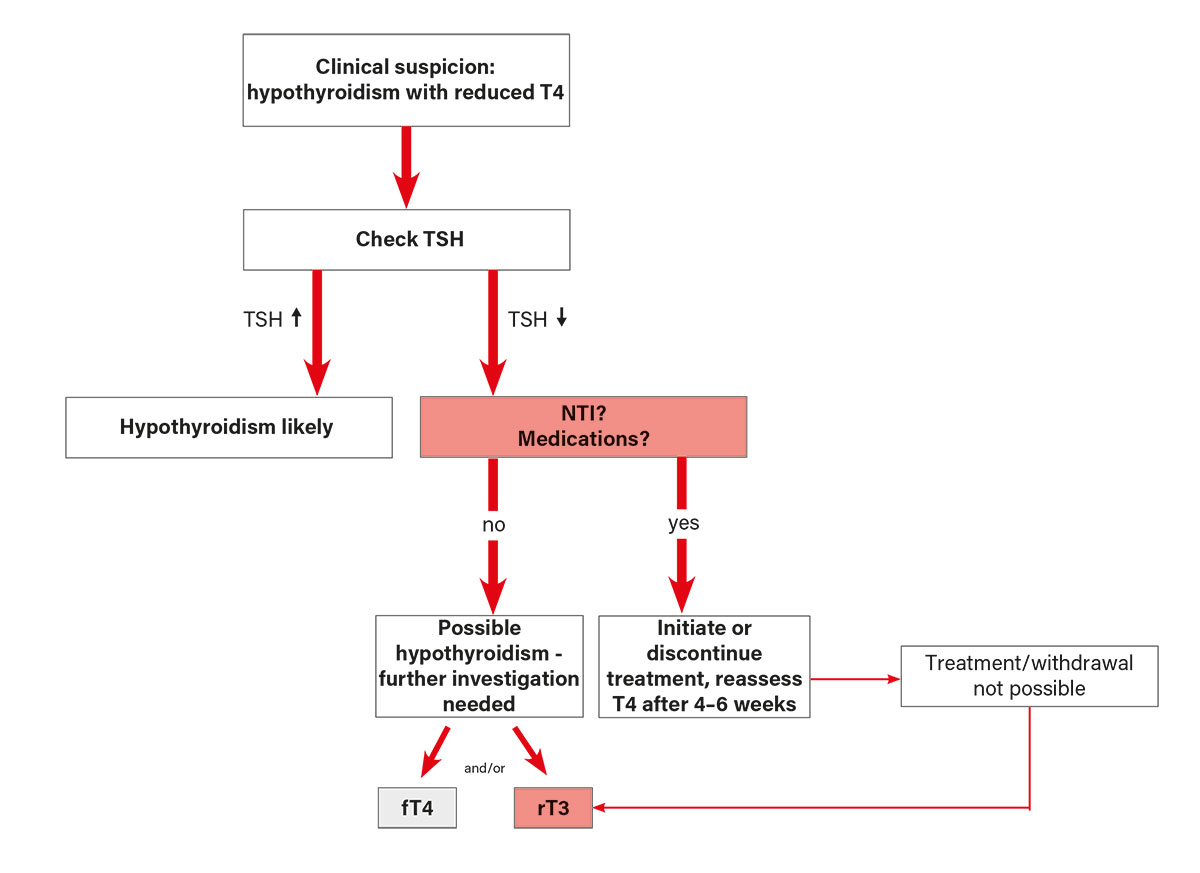
Fig. 3: Initial evaluation of a reduced T4 concentration in blood
Image source: J. von Luckner
The Diagnostic Pitfall: NTI and Methodological Limitations
In a typical case, the diagnosis of canine hypothyroidism is based on the combination of compatible anamnesis, clinical signs, haematological and biochemical findings, together with a T4 concentration below the reference interval and a simultaneous increase in TSH.
However, this pattern is not present in all cases in which hypothyroidism is suspected.
Many diseases can secondarily suppress thyroid hormone concentrations without any functional and/or structural thyroid abnormality. This so-called euthyroid sick syndrome (ESS or NTIS) is characterised by low T4 and/or fT4 concentrations with normal TSH. Interpreting such findings is problematic without further diagnostic work-up.
Additional challenges arise from breed-specific lower iodothyronine concentrations (e.g. Greyhounds, Basenjis) and from the interference of binding proteins or autoantibodies (thyroglobulin-, T3-, T4-autoantobodies) with routinely used immunoassay kits. Moreover, various medications (e.g. glucocorticoids, phenobarbital, sulphonamides) can also influence thyroid parameters.
LC-MS/MS: A Potential New Reference Method
LC-MS/MS has been established as a highly precise analytical technique. Unlike immunoassays, LC-MS/ MS enables the direct and specific quantification of T4, T3 and rT3 without interference from autoantibodies or medications. This makes it particularly valuable in diagnostically challenging cases. For example, while immunoassays can yield falsely low or falsely high results in the presence of thyroglobulin autoantibodies, LC-MS/MS provides a reliable representation of the actual hormone concentration.
At Laboklin, a method for the measurement of T4, T3 and rT3 using LC-MS/MS has been established and validated for veterinary medicine as part of a doctoral thesis. This allows for highly specific diagnostics, particularly in unclear cases. It can also be a reliable option for therapy monitoring or in cases of suspected hypothyroidism despite T4 concentrations within the reference range.
When interpreting T3 and T4 values measured by LC-MS/MS the method-specific reference intervals must be taken into account, as they differ from those obtained using other techniques.
Reverse T3 (rT3): Differentiating NTI from Hypothyroidism
rT3 is primarily produced when there is an excess of T4 or when conversion to active T3 is downregulated. In hypothyroidism, only minimal amounts of T4 are available for conversion, resulting in reduced rT3 concentrations. In contrast, NTI typically leads to normal or elevated rT3 levels: sufficient T4 is available, but the physiological demand for T3 is simultaneously markedly reduced (Fig. 1).
Initial studies confirm the diagnostic value of this parameter:
- rT3 < 50 pg/ml, in combination with a low T4 concentration, strongly suggests hypothyroidism.
- rT3 > 109 pg/ml makes hypothyroidism highly unlikely, even when T4 levels are reduced (Fig. 2).
Indication
This parameter is particularly valuable when T4 or fT4 concentrations are low, but no elevated TSH concentration is present to confirm the suspicion of hypothyroidism. This situation may occur in 20–30% of dogs with hypothyroidism, but it more frequently indicates a non-thyroidal illness (NTI).
Previous Experience with the Parameter
An initial multicentre study on rT3 was presented at an international congress (ECVIM) in 2024.
The study demonstrated that healthy dogs, dogs with hypothyroidism, and those with low T4 concentrations secondary to a non-thyroidal illness (NTI) could be reliably distinguished. A cut-off of 50 pg/ml was identified as highly specific for the presence of hypothyroidism, whereas concentrations above 109 pg/ml were incompatible with hypothyroidism. Values between these thresholds represented a grey zone. To establish a reference interval for rT3, Laboklin conducted a study in a larger population of clinically healthy, euthyroid dogs. This study determined a reference interval of 109–533 pg/ml.
In addition to the conducted studies, highly valuable field data have now become available.
Between March 2024 and June 2025, the rT3 parameter was requested 3,052 times at Laboklin, of which 1,887 requests were for rT3 alone and 1,165 were performed as part of a profile or as an add-on to initially requested thyroid parameters.
Among the 491 cases with an rT3 concentration below 50 pg/ml, T4 was also measured in our laboratory in 289 cases. Of these, 92% of the dogs exhibited T4 concentrations below the reference range, confirming the close functional relationship between reverse triiodothyronine and thyroxine.
Only in 22 cases (7.6%) with an rT3 concentration below 50 pg/ml was the T4 concentration within the reference range. This phenomenon can primarily be attributed to the limitations of the immunoassays routinely used for T4 measurement (e.g., Immulite 2000; Siemens, Germany). Falsely elevated T4 results may arise due to the presence of autoantibodies or suboptimal sample quality (haemolytic or lipaemic samples). These interfering factors are well recognised and can complicate the interpretation of results in routine diagnostics.
In 570 dogs with simultaneously low T4 concentrations, rT3 levels were clearly within the normal range (> 109 pg/ml). Such a result does not support a diagnosis of hypothyroidism, but rather indicates a non-thyroidal illness (NTI). Of course, a single measurement of even highly specific laboratory parameters cannot definitively determine that these dogs did not actually suffer from hypothyroidism, but rather from a non-thyroidal illness (NTI). In all cases that we were able to review in personal discussions with the attending veterinarians, the assessment was, however, confirmed.
Previous studies and clinical experience suggest a major advance in canine hypothyroidism diagnostics. The parameter appears to fulfil its promise. It should be regarded as an additional tool in the “hypothyroidism” toolbox. rT3 is not intended as an initial screening parameter, but rather as an add-on to an existing thyroid profile. Accordingly, it should be interpreted in the context of clinical findings as well as other thyroid parameters (Fig. 3).
For further diagnostics, determination of thyroglobulin-, T3-, T4-autoantibodies is available through extended thyroid profiles. Another option is the measurement of T3 and T4 concentrations using liquid chromatography–tandem mass spectrometry (LC-MS/MS), which is not affected by interfering factors such as sample quality or autoantibodies, allowing for more specific and precise results.
Conclusion
The precise diagnosis of canine hypothyroidism requires more than the assessment of T4 and TSH alone. In particular, an rT3 measurement and LC-MS/MS-based analyses provide crucial information in cases of diagnostic uncertainty.
Dr. Jennifer von Luckner, Niklas Wiesner, Dr. Ruth Klein
Our Services Related to Hypothyroidism
- T4, TSH, fT4
- T3, fT3
- rT3
- Thyroid Profile (T4, fT4, T3, fT3, TSH, ATG, T4-AK, T3-AK)
- Hypothyroidism/NTI Profile (T4, fT4, reverse T3, TSH)
- Thyroid Monitoring (T4, TSH, Creatinine, SDMA, ALT, AP, Troponin I)
- Thyroid Mass Spectrometry (T4, T3, rT3 by HPLC-MS/MS)



