Leukaemias are rare in dogs and cats compared to other solid neoplasms. They are difficult to diagnose in the early stages and can easily be confused with inflammation or other diseases. Therefore, in addition to a full blood count and a thorough medical history, additional diagnostic tests are required before the diagnosis of leukaemia can be confirmed.
What is leukaemia?
Leukaemia is a malignant disease of the bone marrow where the uninhibited, clonal proliferation of haematopoietic precursor cells leads to a more or less severe displacement of normal haematopoiesis in the bone marrow (BM).
A distinction can be made between lymphocytic and myeloid leukaemia (affecting erythrocytes, granulocytes, monocytes and thrombocytes).
Depending on their course and the proportion of blasts in the bone marrow and peripheral blood, leukaemias can be divided into acute and chronic. It is important to know the difference between leukaemia and lymphoma.
Both are haematopoietic neoplasms, but they develop in different tissues. Lymphomas typically develop in lymphatic tissue (e.g., lymph nodes and the lymphatic system). As in human medicine, it is sometimes difficult or impossible to differentiate precisely between lymphoma and lymphatic leukaemia, even with a detailed preliminary report.
Epidemiology
Both genetics and environmental influences play a role as risk factors for the development of leukaemia and lymphoma.
Familial, genetic relationships have been described in dogs (e.g., Golden Retriever, Gordon Setter, Portuguese Water Dog, Rottweiler and Irish Setter) and in oriental breeds of cats, such as Siamese cat. Environmental factors (e.g., exposure to cigarette smoke) and infectious diseases (FeLV) can also contribute to the development of haematopoietic neoplasia.
-

- Image source: envatoelements

-
-
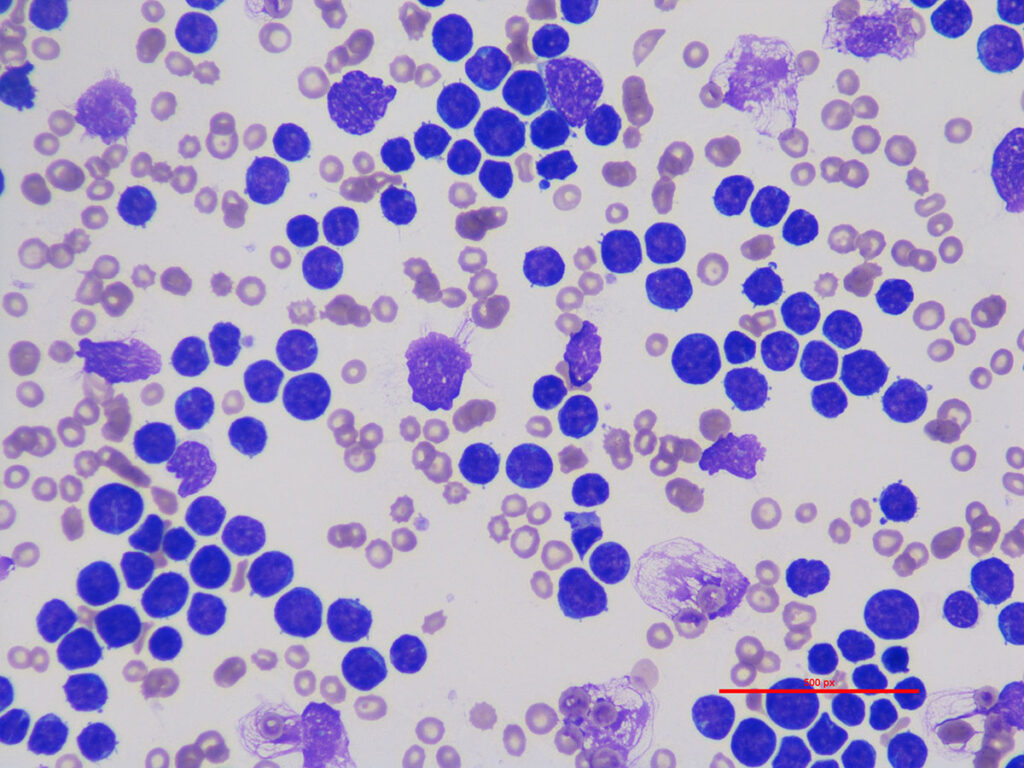
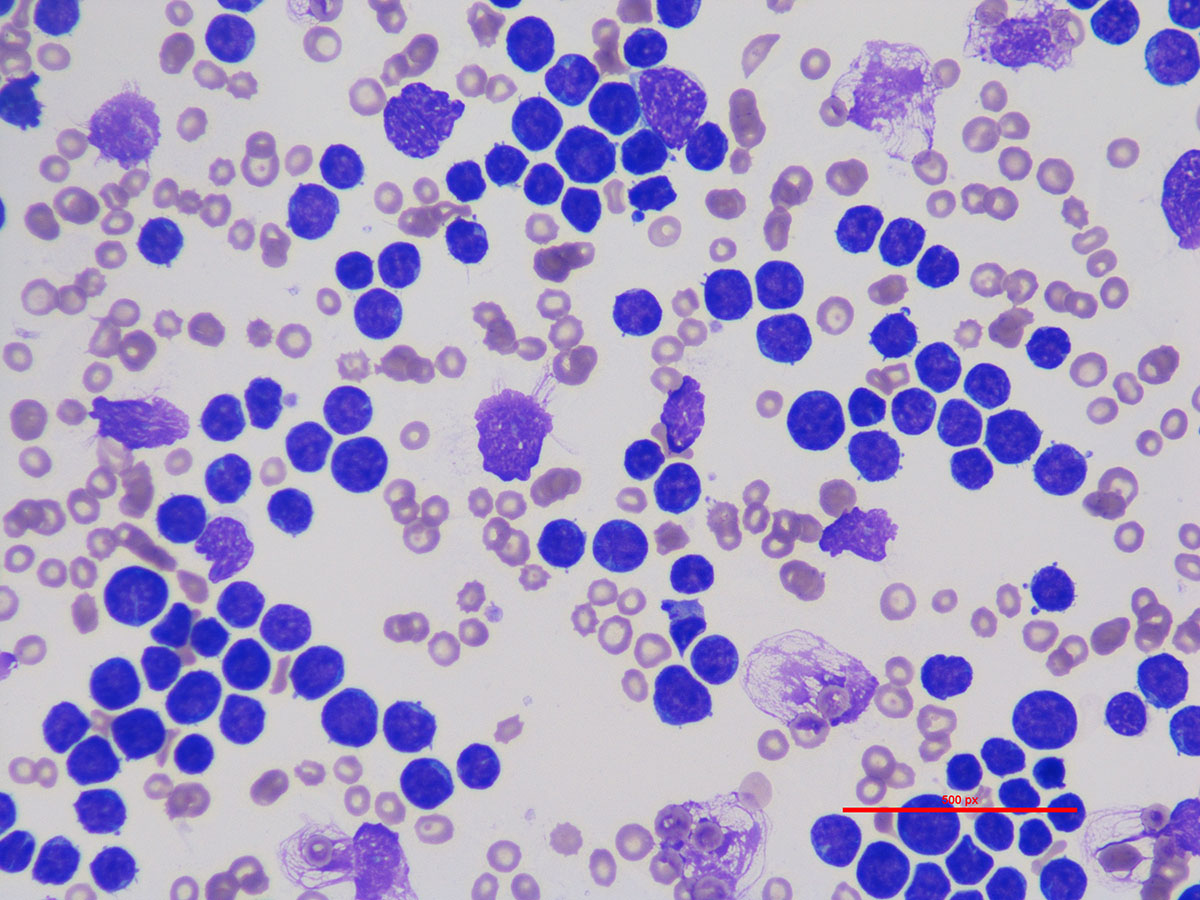
Lymphatic leukaemia, dog. Wright-Giemsa staining,
500x magnification with immersion oil.
Image Source: Laboklin
-
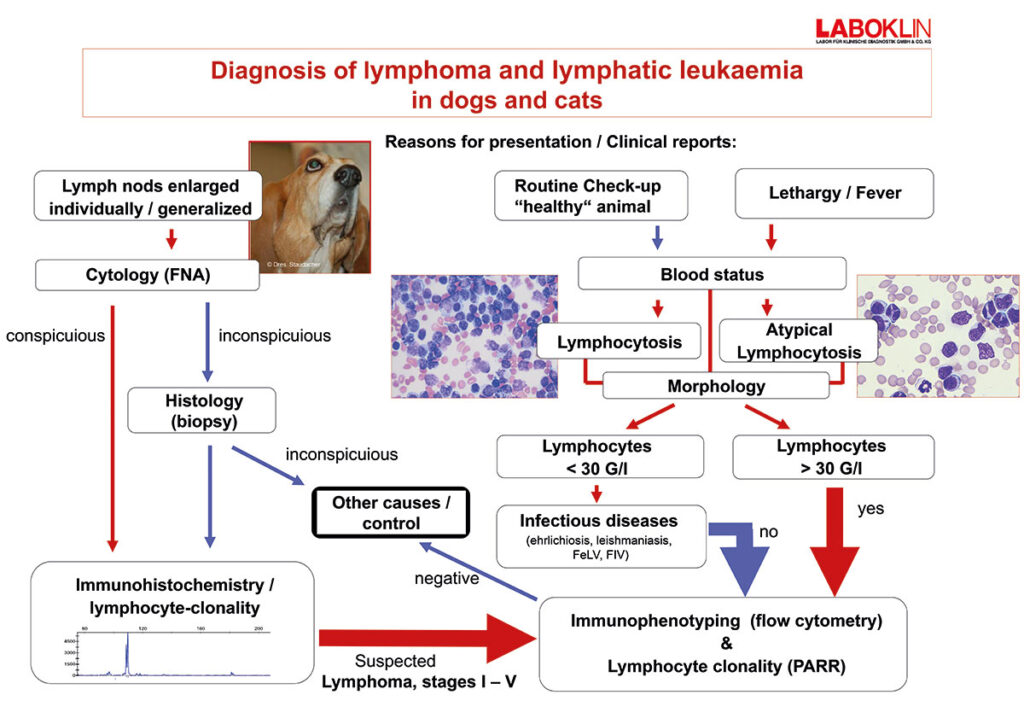
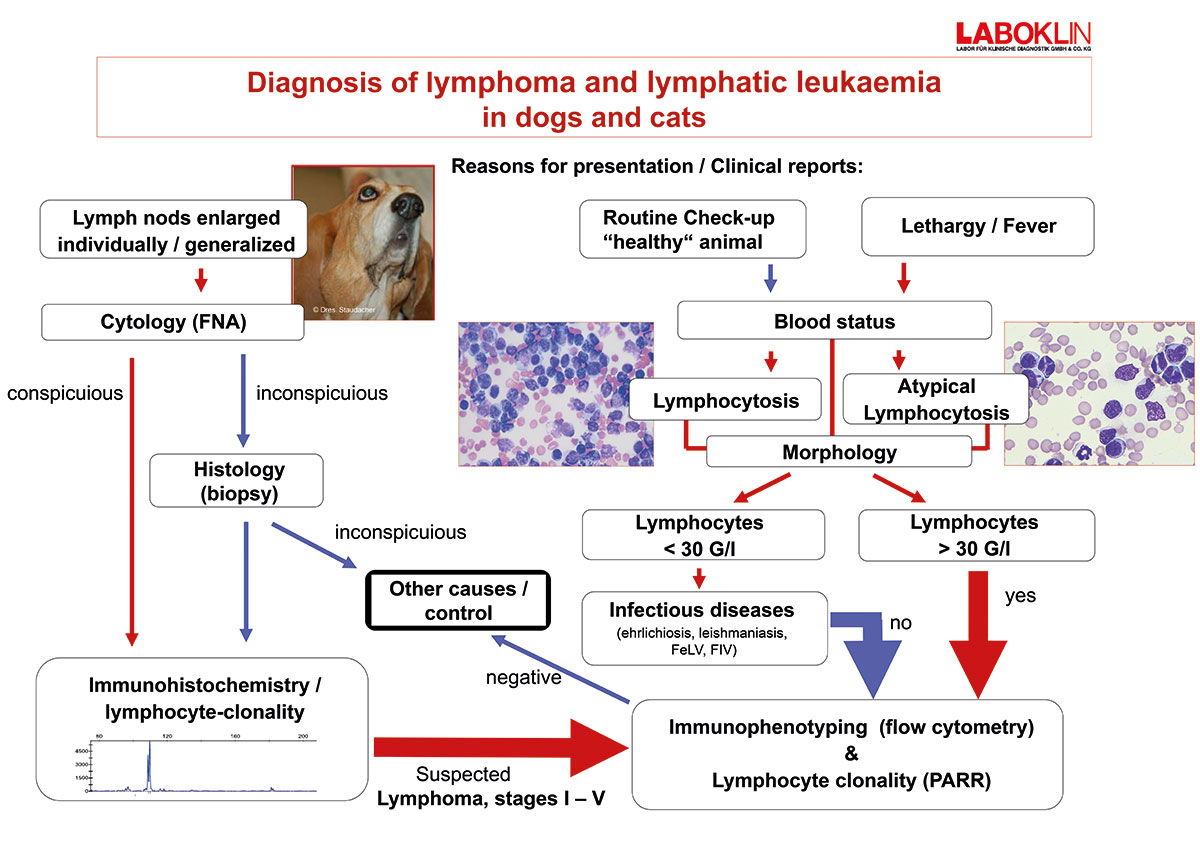
- Diagnosis of lymphoma and lymphatic leukaemia in dogs and cats
It is known from human medicine that leukaemia can be triggered by exposure to various carcinogens, such as benzene and phenylbutazone, as well as radiation, however, in veterinary medicine, there is currently limited data available in this area of research. Leukaemia predominantly affects middleaged animals, regardless of sex.
Clinic
The clinical appearance of haematopoietic neoplasia varies greatly and depends on the localisation of the disease, affected organs, and the presence of paraneoplastic inflammation.
Patients with myeloproliferative neoplasms, chronic lymphocytic leukaemias, and lymphomas are often asymptomatic at the beginning.
During the course of the disease, non-specific changes can occur. These include:
- Lethargy
- Reduced appetite
- Gradual weight loss
- Organ changes as the disease progresses (splenomegaly, hepatomegaly, lymphadenomegaly)
In contrast, patients with acute leukaemia usually show severe clinical signs:
- Acute loss of condition
- Fever
- Inappetence
- Weight loss
- Vomiting
- Diarrhoea
- Organ changes (splenomegaly)
Laboratory reports
Leukaemia is often an incidental finding.
Changes in the white cell count in the form of leukocytosis are among the most prominent findings. Leukocytosis can vary in degree and is triggered by an increase in the affected cell series.
Lymphocytosis are the most frequently observed form and can range from mild to severe. As a rule, the animal’s condition progressively deteriorates with increasing duration of the disease.
Other typical changes include anaemia and thrombocytopenia.
Classification
Leukaemias are classified according to the stem cell lineage from which the neoplasia originates.
A distinction is made between myeloid and lymphatic leukaemias, which can further be subdivided into acute and chronic types.
Myeloproliferative neoplasms have their origin in the precursors of erythrocytes, granulocytes, monocytes, or thrombocytes.
Lymphocytic leukaemias have their origin in precursors of T or B lymphocytes or natural killer cells.
Lymphoproliferative neoplasms
Lymphatic leukaemias can be further classified based on the cell type, the number of cells in circulation, and the stage of the disease.
A distinction is made between acute lymphoblastic leukaemia (ALL) and chronic lymphocytic leukaemia (CLL). This classification system is based on the severity of the disease, the cell morphology, the immunophenotype, and genetic changes in the cells. While the lymphocytes in CLL are morphologically similar to normal small, mature lymphocytes, immature, medium-to-large lymphoblasts are found in ALL.
Myeloproliferative neoplasms (MPN)
Myeloproliferative neoplasms (MPN) occur very rarely in dogs and cats. They are usually indolent and slowly progressive but can develop into aggressive acute myeloid leukaemias (AML).
In human medicine, only a few hundred cases of chronic neutrophil or eosinophil leukaemia have been described. Similarly, only isolated cases have been described in dogs and cats. These individual cases are always a diagnosis of exclusion, made after careful diagnostics, including bone marrow cytology and repeated blood counts. Reactive processes and inflammation occur much more frequently and must therefore be ruled out with certainty.
Acute myeloproliferative neoplasms
Acute myeloid leukaemia (AML) is a heterogeneous, aggressive neoplasia of the haematopoietic stem and progenitor cells. Acute myeloid leukaemias are classified according to their cellular origin and immunophenotype and are categorised into different subtypes: AML-M0, AML-M1, AML-M2, AML-M2B, AML-M4, AML-M5, AML-M6, and AML-M7.
Diagnostics
Depending on the changes in the blood count and the preliminary report, the diagnosis of leukaemia can vary in complexity due to the many different entities.
The following are necessary for the diagnosis and classification of leukaemia:
- Thorough anamnesis
- Signalement
- Complete full blood count
- Clinical-chemical organ parameters
- Travel history (ehrlichiosis? leishmaniasis?)
- Vaccination status?
- Outdoor cat? (FeLV)
- Cytomorphology (peripheral blood, bone marrow)
- Immunophenotyping using flow cytometry
- Lymphocyte clonality analysis
- Cytochemical staining
Morphological cell assessment plays a definitive role in the diagnosis of leukaemia, which is why highquality, fresh smears are absolutely essential.
The cell morphology provides a preliminary indication of the possible origin of the neoplasia. Cell differentiation, the proportion of dysplastic changes, and the number of blasts are used for further pre-differentiation. Further tests, such as immunophenotyping and clonality testing, can then be carried out.
Immunophenotyping is a procedure in which the cell lineage is determined using antibody staining in fluids (e.g. peripheral blood, bone marrow, or lymph node aspirate or biopsy). This technique not only allows differentiation between myeloid and lymphatic leukaemia but also enables the distinction between acute and chronic leukaemia in dogs.
At the genetic level, B and T lymphocytes can be identified. As the disease progresses, the origin of lymphatic leukaemia can often be differentiated into T helper cells, cytotoxic T cells, or B cells.
This enables more precise prognostic assessments.
Lymphocyte clonality testing (PARR = PCR for antigen receptor rearrangements) can be used to detect a monoclonal lymphocyte population using DNA from blood, aspirates, smears, and tissue samples.
At the genetic level, B and T lymphocytes can be distinguished.
Conclusion
Leukaemias occur in dogs and cats but are rare. If myeloproliferative neoplasia is suspected, inflammation must be ruled out beforehand.
Further examinations, such as cytomorphology, immunophenotyping, and clonality tests, are required for classification.
Dr. Annemarie Baur-Kaufhold



