FeLV and FIV are often neglected as it is often assumed that they are rare.
However, they play a role that should not be underestimated. Even in countries where the disease prevalence is presumed to be low, infection with either FeLV or FIV must always be taken into consideration. Especially if there are non-specific signs of illness such as anaemia, fever and lethargy. Not least because – especially for FeLV – infection is of prognostic relevance.
Screening clinically healthy cats is important when introducing a new cat into a household or colony, as a pre-operative measure, as a health profile in blood donors or when importing a cat from an area of high prevalence (e.g. some southern and eastern European countries) into one of low prevalence.
FeLV
The feline leukaemia virus is an RNA virus from the retrovirus family. It is able to transfer its genome into the DNA of host cells (provirus). Transmission usually occurs oronasally via virus-containing secretions such as saliva, nasal secretions, milk, urine or faeces. Vertical transmission from the mother to the kitten is possible.
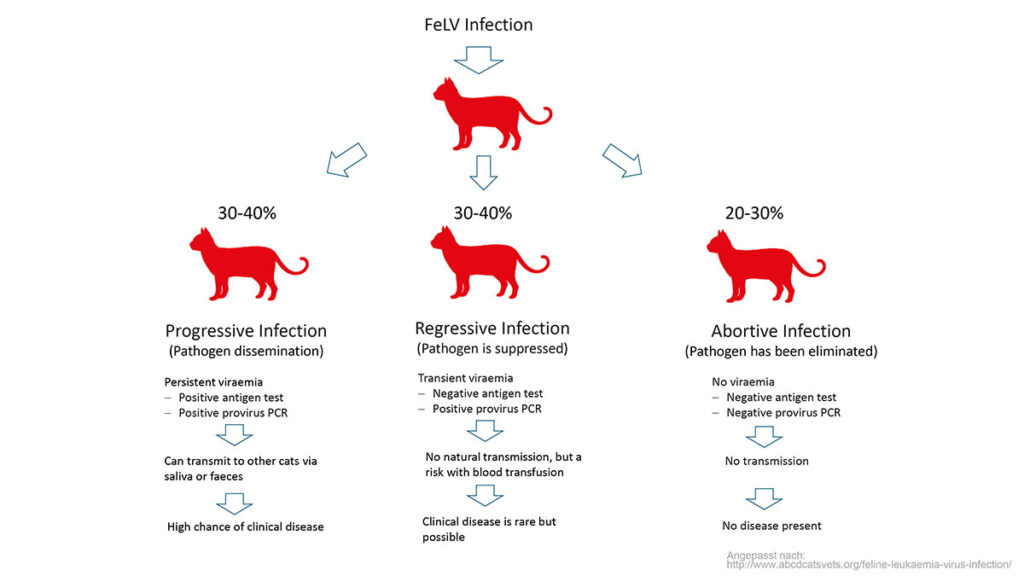
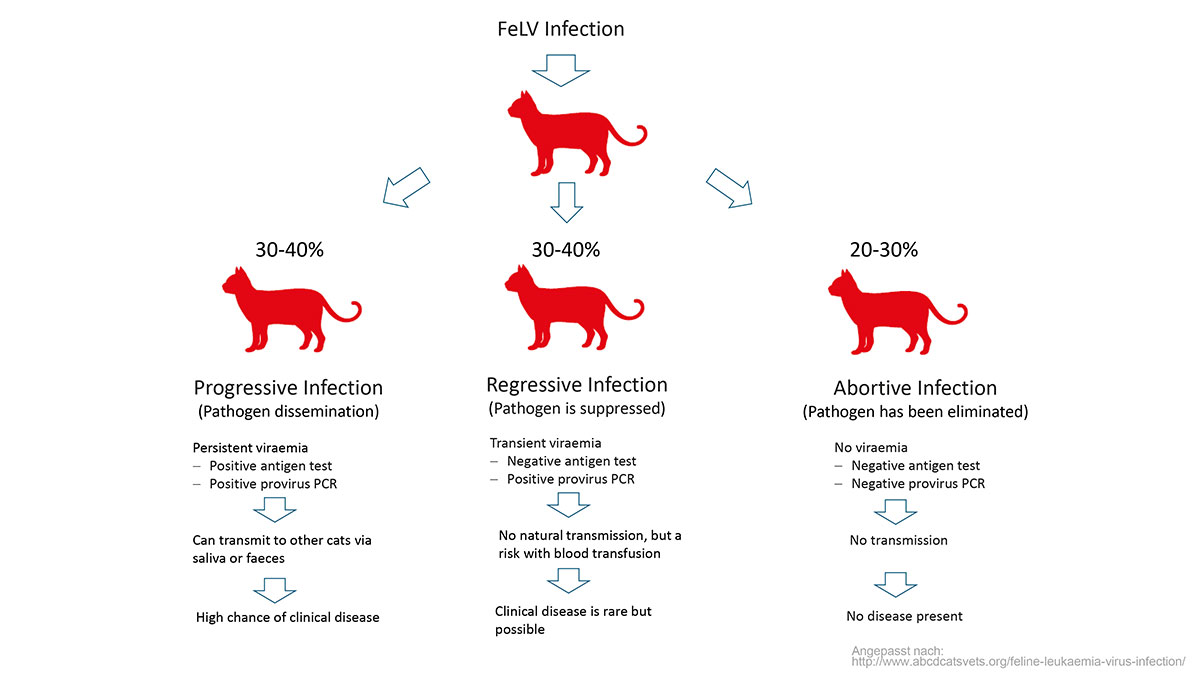
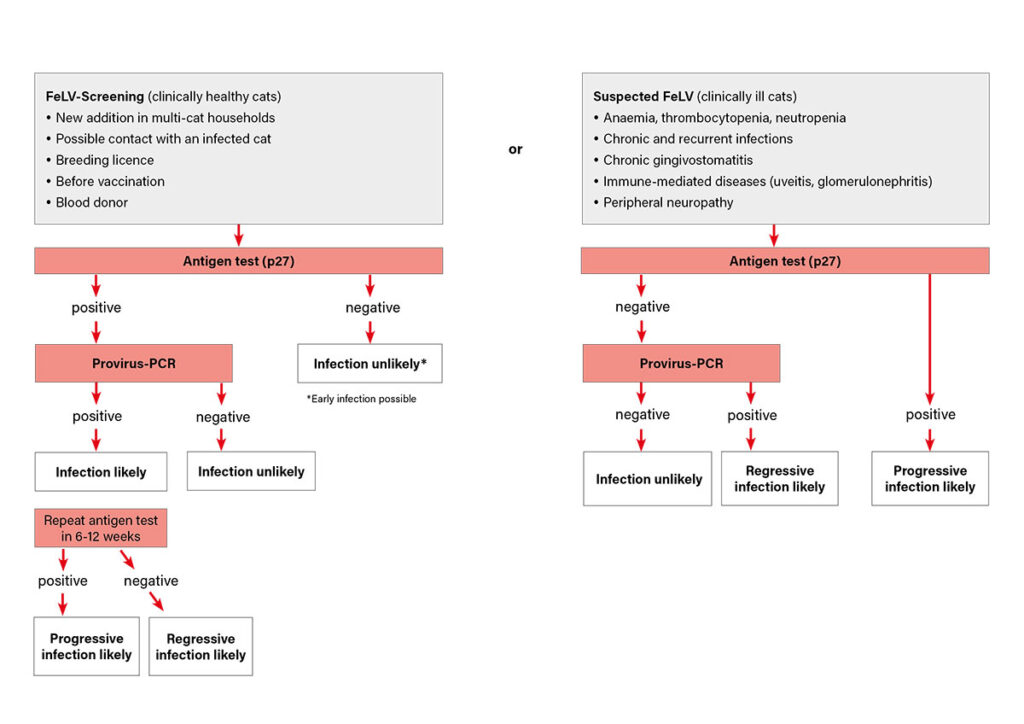
After an infection, three different scenarios can occur (Fig. 1):
- Progressive infection: Both the full virus and the provirus are present. Circulating antigen is detectable.
- Regressive infection: The pathogen is only detectable as a provirus incorporated into the DNA, there is no circulation of antigen.
- Abortive infection: The cat succeeds in eliminating the pathogen from the body.
Clinical signs are primarily seen in progressive infections, but have also been described in regressive infections. Various organ systems can be affected, FeLV manifests itself in a variety of clinical signs. The most common clinical signs of FeLV infection are anaemia and lymphoma. Uveitis is also relatively common. Immunemediated diseases such as immune haemolytic anaemia, glomerulonephritis and polyarthritis have been described.
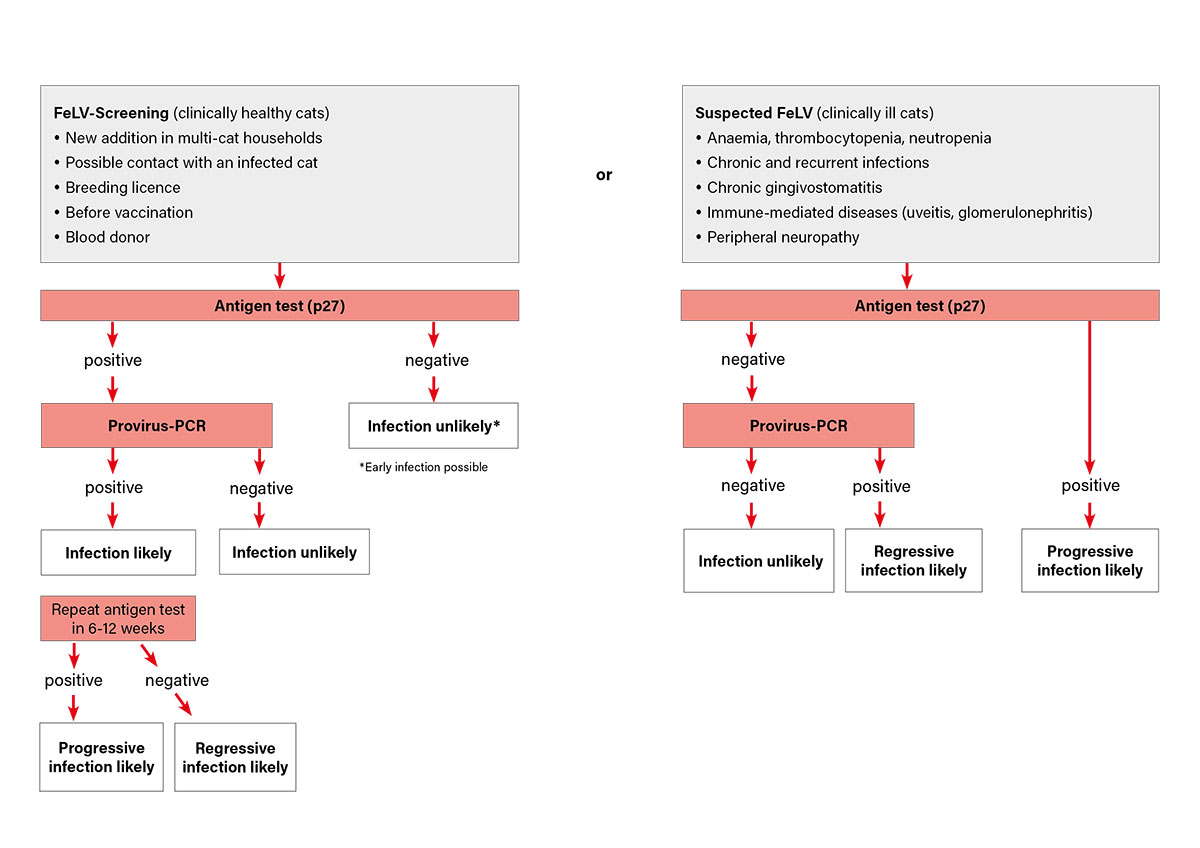
Point-of-care antigen (POC) tests are available as a screening test for FeLV infection. These detect the p27 antigen of the pathogen circulating in the blood (only present in progressive disease). In clinically healthy cats, a negative result excludes an infection with a high probability as long as the prevalence in the region the cat lives in is low. However, in the case of very early infection (< 21 – 30 days), it is possible that no antigen is yet circulating. As the probability of a false positive test result increases with low prevalence, as is the case for FeLV in many northern countries, a positive POC test should be verified by means of a confirmatory test. This is usually done by checking for the presence of provirus using PCR. Alternatively, retesting by ELISA can be carried out in an external laboratory.
-
-
Fig. 1: Schematic representation of the possible progression forms of FeLV
Image source: Laboklin
-
-
Fig. 2: Simplified representation of testing options for suspected FeLV
Image source: Laboklin
-
-
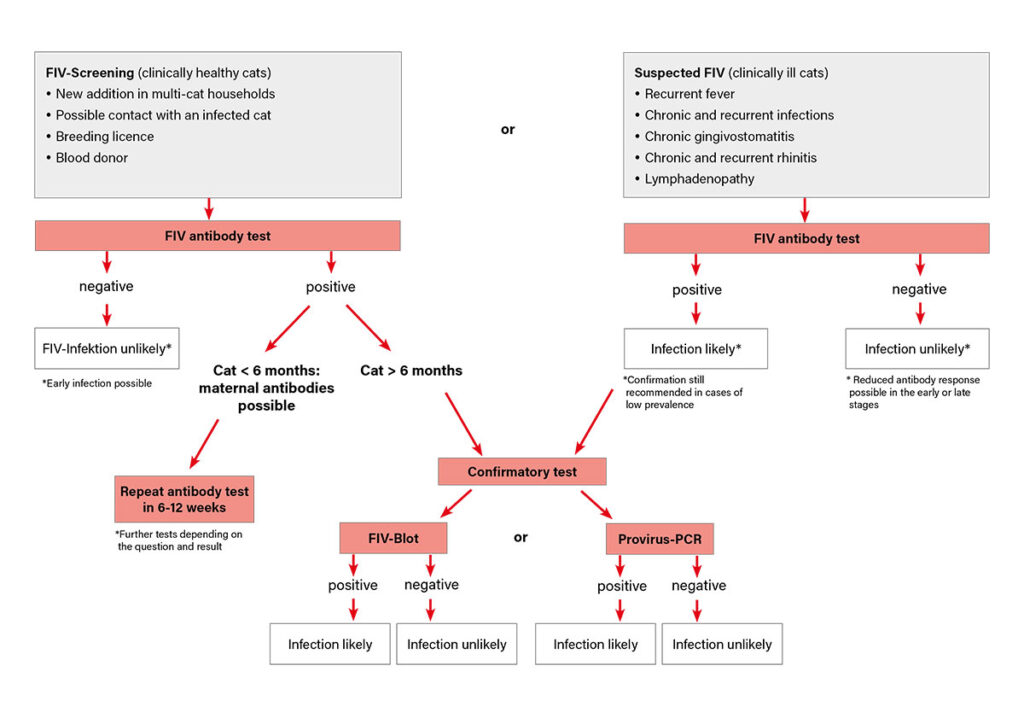
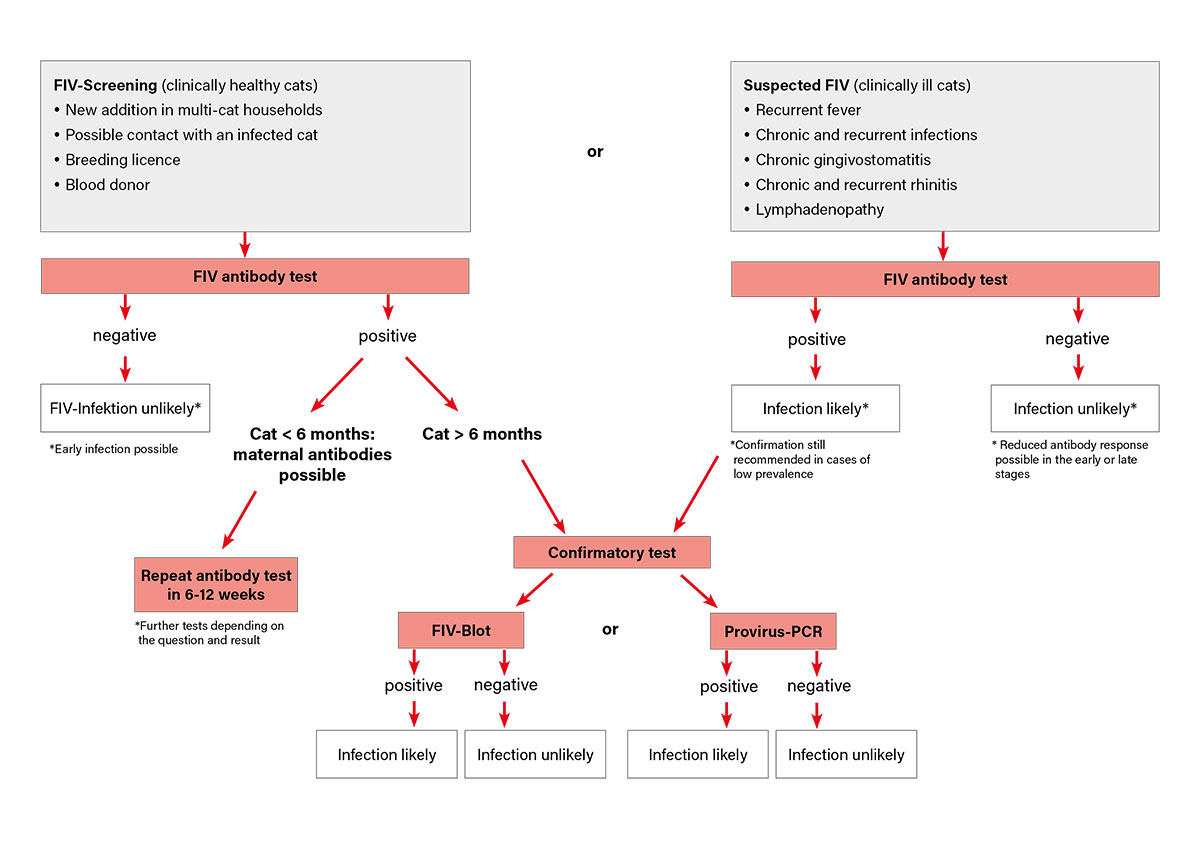
Fig. 3: Simplified representation of testing options for suspected FIV
Image source: Laboklin
If there is clinical suspicion of FeLV infection but the screening test result is negative, further testing is recommended as regressive infection is possible. In regressive infection no free antigen is detectable in the blood and the antigen test is therefore negative despite the presence of infection (Fig. 2). If progressive FeLV infection is present, the prognosis is guarded. With progressive infection, the development of clinical signs and death can be expected within three years. There are, however also long-term survivors.
The administration of interferon appears to reduce secondary infections and prolong survival times. Regressively infected cats usually remain asymptomatic in the long term. However, reactivation of the infection is possible.
Monitoring of FeLV-infected patients is of major importance. They should undergo regular clinical examinations, including blood tests to identify any secondary concerns (anaemia, lymphoma, other infections). Routine vaccination against the common infectious diseases is recommended.
FeLV-infected cats should be kept as indoor-only cats for not only their own protection (secondary infections) but to stop the transmission to other cats.
The most important questions regarding FeLV:
- There is clinical suspicion of FeLV infection but the antigen test is negative. Should I run the provirus test or should antigen always be circulating in a sick cat?
As a rule, the FeLV antigen will also be circulating if the cat is clinically ill.
However, there are some cases that are clinically ill with an FeLV infection but are antigen negative. These can usually be identified by provirus detection (PCR). - How often is a regressive FeLV infection reactivated? Is this still possible years later?
Outbreaks of the disease are possible with a regressive form of the disease. This can even occur several years after infection.
Unfortunately, there are no exact figures on how often this happens. In one study, reactivation was observed in 2 out of 37 regressively infected cats. - Can a regressively infected cat transmit the disease?
Regressively infected cats do not excrete the virus in their saliva or faeces and therefore do not transmit FeLV naturally.
However, it should be noted that transmission via blood transfusion is possible. Blood donors should therefore not only be screened using an FeLV antigen test, but should also be tested using provirus PCR. - When should a cat with a positive antigen test for FeLV be retested (to check whether the cat has become regressive)?
An initial viraemia can turn into a regressive infection in which only provirus is detectable. The antigen test then becomes negative. This is usually the case within 12 weeks of infection, but in rare cases can happen later (maximum documented time is one year). Antigen-positive cats should be separated from healthy cats and retested at 3 – 6 week intervals. If they become antigen-negative, they can be reunited with other cats.
FIV
The feline immunodeficiency virus is an RNA virus from the retrovirus family with the ability to integrate its genome into the DNA of host cells.
Transmission is not quite as rapid as with FeLV; cats usually become infected via bite wounds.
Transplacental infection of kittens is possible. Transmission during mating has not been described, although virus has been detected in the semen of infected males. Bite injuries during mating are possible.
An initial infection phase, which can be accompanied by mild clinical signs such as fever or neutropenia, is followed by a subclinical phase. The subclinical phase can last a lifetime. Whether transition to the clinical phase occurs depends on the virus isolate, immunity and age of the cat at the time of infection. Typical clinical signs caused by FIV usually are induced by dysregulation of the immune system. Chronic gingivostomatitis, chronic rhinitis, lymphadenomegaly, glomerulonephritis and weight loss are common. Viral, bacterial and protozoal secondary infections are to be expected.
An increased incidence of neoplasia (lymphoma, squamous cell carcinoma) has been described. Behavioural changes and a disturbed sleep rhythm may also be present.
Cats remain infected with FIV for life. However, many live with the infection into old age. This distinguishes FIV infection from FeLV infection.
Very good care (including regular dental hygiene and protection against secondary infections) and good clinical and laboratory diagnostic monitoring are essential for keeping the patient healthy. Blood count, blood chemistry and urine should be checked every six months. Depending on the findings, protein electrophoresis and determination of the acute-phase protein serum amyloid A (SAA) can also be helpful. An altered ratio of the so-called CD4/CD8 T lymphocytes may indicate an existing immune dysfunction.
To check for FIV infection, blood testing for FIV-specific antibodies is usually carried out (Fig. 3). This can be done using a POC test. As the infection persists for a lifetime, antibody detection is well suited for diagnosis. Seroconversion usually takes place within 2 – 4 weeks. In some FIV-infected cats, however, antibody production may be delayed by weeks to months, while the cats are already able to transmit the pathogen.
If the cat is living in an area with a low prevalence of FIV, a positive test should be confirmed by a second (non-POC) test. The so-called blot method (Western blot, line blot) is suitable for this purpose. In contrast to POC tests, these methods enable the detection of various antibodies directed against FIV-specific antigens. A blot test is only considered positive for an FIV infection if antibodies against at least two (preferably three) antigens can be detected. In case of doubt, the detection of provirus by PCR can also be considered but negative results are not exclusive for FIV (see below). Kittens from an FIV-infected mother can have maternal antibodies without being infected themselves. As a general rule, maternal antibodies do not persist for longer than 16 weeks, but there are cases where they may be detected up to 6 months of age. If a 16-week-old kitten is positive for FIV antibodies, retesting is recommended after 2 – 3 months. A positive antibody test result that persists after 6 months of age is regarded as proof of infection. Positive test results can also occur up to 6 months after vaccination. However, vaccines against FIV are not authorised in Europe at the moment. Negative results despite infection can occur in the first 60 days after infection and in the final stages of infection.
The most important questions regarding FeLV:
- At what point after possible transmission can an FIV infection be safely ruled out?
If there is the possibility that a cat has been infected (e.g. because it has escaped), the recommendation is to quarantine it for three months. Only if the antibody test is negative at the end of this period can it be assumed that no infection has taken place. - What is recommended if there is a questionable antibody titre that persists even after two weeks?
In such cases, it is advisable to ask for an FIV blot. If this is negative, an infection is unlikely. If the FIV blot also gives questionable results, a PCR for provirus can be carried out. However, this is only meaningful in a positive case (= FIV infection present). PCR cannot be used to rule out the infection with certainty. Determination of the CD4/CD8 quotient may allow further classification under certain circumstances. - Why is a negative PCR not ruling out infection with certainty?
The PCR assays currently available detect FIV virus of group A (predominant in Europe) with a high sensitivity and specificity. However, there is variable sensitivity for other groups of the virus. In addition, there is a relatively high strain variability and mutation rate, i.e. the virus can show differences within a group. This means that not every infection can be detected by PCR. Positive results are therefore conclusive. However, a negative PCR result does not rule out an FIV infection with certainty.
Dr. Jennifer von Luckner, Theresa Marquar
| Our services at a glance | ||
| FeLV-Antigen | Screening
Suspected FeLV |
|
| FeLV-Provirus-PCR
FIV antibodies (ELISA) |
Confirmation of a positive FeLV antigen test Detection of regressive infection in a negative antigen test Screening of blood donorsIn questionable cases, the test should be repeated after 2–4 weeks. An FIV blot should be performed to confirm positive results. |
|
| FIV-PCR | Qualitative: Detection of provirus Quantitative: Determination of proviral load |
|
| FIV-Blot | For verifying unclear/borderline results or confirming positive results from previous tests. This antibody detection is performed using a line blot and is highly specific due to the use of three different antigens. | |
| FIV-Monitoring | ALT, GLDH, ALP, BUN, Creatinine CD4/CD8 (sample age < 48 h) FIV PCR (quantitative) + Blood count |
|
| Cellular immune status | Blood count Determination of B cells (CD21+), T cells (CD3+, CD5+), T helper cells (CD4+), and cytotoxic T cells (CD8+) |
|