The LABOKLIN expert panels, featuring exciting topics and outstanding specialists, are extremely popular. We have selected the most important answers to your questions on the topic of lymphoma.
Our team of experts consisted of: Prof. Dr Carla Rohrer Bley, Dipl. ACVR, Dipl. ECVDI (Radiation Oncology), Master of Applied Ethics, Director of Clinical & Translational Oncology, Vetsuisse Faculty, University of Zurich, Switzerland; Dr Heike Karpenstein-Klumpp, German Specialist (Fachtierarzt) radiology/imaging and internal medicine), Zentrum für Tiergesundheit Baden-Baden, Germany; Dr Sandra Lapsina, Dipl. ECVCP, LABOKLIN, Germany; Dr Jarno Schmidt, Dr. med. vet., Dipl. ECVIM-CA (Oncology), MRCVS, German Specialist (Fachtierarzt) internal medicine, M.A. (mediation & conflict management), IVC Evidensia Tierklinik Hofheim, Germany.
Prof. Dr Rohrer Bley provides an introductory overview. She explains that lymphoma is a neoplastic transformation of lymphocytes, which can occur either locally or in a generalised form.
Different types of lymphoma are classified based on the organs affected. In dogs, generalised, multicentric lymphoma involving the lymph nodes is particularly common, while mediastinal, cutaneous, and intestinal lymphomas occur less frequently.
In cats, gastrointestinal lymphomas are especially prevalent, followed by lymphomas of the kidneys, nasal cavity and mediastinum. Another important classification is based on the cellular origin, e.g. B-cell or T-cell lymphoma.
When asked about breed predispositions, Dr Schmidt explains that, in principle, all breeds can be affected. However, certain breeds appear to be disproportionately predisposed. There are also regional differences: for example, in the USA, Golden Retrievers are frequently mentioned, whereas in Europe, Boxers, Dobermanns and Bernese Mountain Dogs are more commonly affected.
Dr Lapsina reports that prognosis is influenced by the cell type. For instance, the prognosis for T-cell lymphomas is often poorer than for B-cell lymphomas in canine multicentric lymphoma.
Moreover, the subtype can also have an impact. Therefore, it may be advisable to perform further classification of the lymphoma (e.g. via immunophenotyping using flow cytometry or immunohistochemistry) once the diagnosis has been confirmed. Dr Schmidt supports this view and adds that certain anatomical forms are associated with a less favourable prognosis (e.g. feline renal lymphoma, canine intestinal lymphoma). However, alongside aggressive (high-grade) lymphomas, there are also indolent or low-grade variants for which the prognosis may be considerably better (e.g. feline small-cell intestinal lymphoma).
The participants would like to know which findings might raise suspicion of lymphoma. Dr Karpenstein-Klumpp looks for enlarged peripheral lymph nodes in dogs. She also pays close attention to dogs with an enlarged spleen on palpation, or cats with renomegaly. In cats, she routinely performs careful compression of the cranial thorax. The otherwise highly mobile thoracic wall in cats becomes rigid in the presence of large mediastinal masses. Other potential indicators prompting an investigation for lymphoma include chronic weight loss, polyuria/ polydipsia (PU/PD), or fever of unknown origin.
Dr Lapsina notes that blood findings are generally non-specific. However, changes that should prompt consideration of lymphoma as a differential diagnosis include non-regenerative anaemia, thrombocytopenia, lymphocytosis, eosinophilia, hypercalcaemia, hyperglobulinaemia, and increased concentrations of acute phase proteins (serum amyloid A in cats, C-reactive protein in dogs).
Lactate dehydrogenase (LDH) holds a special place — it can be markedly elevated in lymphoma and may even be prognostically relevant.
Tumour markers can also be assessed. However, Dr Lapsina notes that the currently available markers are more suitable for screening in clinically healthy dogs and for monitoring during follow-up. Thymidine kinase and nucleosomes are of particular relevance.
Thymidine kinase levels increase during cell proliferation and are elevated in cases of lymphoma, but may also rise in inflammatory conditions. This marker is of interest because, in canine multicentric lymphoma, elevated thymidine kinase levels during or after treatment may indicate an early relapse — even before lymphadenomegaly becomes clinically apparent. Therefore, measuring thymidine kinase before the start of therapy can be useful for monitoring thereafter.
Nucleosomes, which are released into the blood during cell death, may also serve as a screening tool. An increased concentration in a clinically healthy dog can suggest the presence of a tumour. However, it is important to recognise that interpretation becomes challenging in dogs with fever or other clinical signs, as the marker does not differentiate between inflammation and neoplasia.
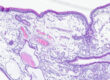
Dr Karpenstein-Klumpp provides a concise yet excellent overview of the indicative findings in abdominal sonography. In dogs with multicentric lymphoma, she often identifies an enlarged spleen with well-defined, hypoechoic areas — commonly referred to as a “moth-eaten” appearance — along with large, hypoechoic, round abdominal lymph nodes. Hepatic lymphoma, on the other hand, tends to show less characteristic changes and is often difficult to detect. Renal lymphoma in cats typically presents as renomegaly with an irregular surface and a hypoechoic peripheral rim. Large-cell lymphoma of the gastrointestinal tract in both dogs and cats is usually characterised by focal, markedly hypoechoic thickening of the intestinal wall, accompanied by complete loss of normal layering. Associated abdominal lymph nodes are generally enlarged, round, and hypoechoic. In contrast, the small-cell or low-grade intestinal lymphoma frequently seen in cats is sonographically indistinguishable from inflammatory bowel disease. The muscularis layer of the intestine is often thickened, as is also seen in inflammatory conditions, but the normal layering remains intact.
While the intestinal lymph nodes are enlarged and typically show reduced echogenicity, they do not exhibit the pronounced hypoechogenicity and altered morphology characteristic of high-grade lymphoma.
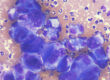
Dr Lapsina emphasises that cytology is a central diagnostic tool in the evaluation of lymphoma.
If cytology reveals a highly uniform (monomorphic) lymphocyte population and/or the lymphocytes exhibit atypia, there is a strong suspicion of lymphoma. In this context, Prof. Dr Rohrer Bley strongly advises against initiating any “ diagnostic” therapy with glucocorticoids, as subsequent diagnostic procedures — particularly cytology — are usually no longer reliable under such treatment.
Dr Lapsina offers valuable tips for performing a lymph node puncture and preparing a smear that can be reliably assessed. Ideally, the puncture should be performed without aspiration to avoid excessive blood contamination and an overly dense cellular smear. Lymphoma often releases a high number of cells, which can overlap on the slide, making interpretation difficult. A good technique is to use only the needle without an attached syringe. A smaller needle bore (e.g. 22 gauge) is recommended. The material placed on the slide should be spread very gently with a second slide, as lymphoma cells are fragile and easily destroyed by pressure, rendering them unsuitable for cytological evaluation. If multiple lymph nodes are enlarged, it is advisable to choose the prescapular or popliteal nodes for sampling.
Mandibular lymph nodes are frequently affected by oral cavity infections, which may complicate the diagnosis. Additionally, they are often mistaken for the salivary glands during sampling.
Cytology can be followed by immunophenotyping using either flow cytometry or PARR (PCR for Antigen Receptor Rearrangement).
Dr Lapsina explains the purpose and application of each method. PARR is a PCR-based test used to determine whether the lymphocytes present are derived from a single clone or from different lineages. It provides a simple yes/no answer to the question of whether the sample is consistent with lymphoma, and is primarily used when cytological findings are inconclusive. PARR is a robust method that can be performed on almost any material, including already stained cells on a slide. In contrast, flow cytometric immunophenotyping does not merely confirm the presence of lymphoma but also allows for subtype classification, which is crucial for prognosis and treatment planning. However, this method requires fresh, liquid samples. Suitable specimens include blood and cell aspirates rinsed in a 50:50 mixture of 0.9% NaCl and patient serum.
Alternatively, immunohistochemistry can be performed on tissue biopsies. This is the most reliable approach but is more time-consuming and invasive.
Now the participants are interested in the opinions of the experts on staging. Dr Schmidt reports that canine multicentric lymphoma is classified into five stages. Most dogs with multicentric lymphoma are presented in stage 3 (generalised peripheral lymph node involvement) or 4 (liver and spleen also altered). Interestingly, there is no prognostic difference between the two stages. In the case of typical sonographic findings (e.g. moth-eaten spleen), Dr Schmidt does not usually insist on a cytological examination of spleen and liver.
However, he always recommends a complete haematology, including the assessment of a freshly prepared blood smear. If many large and/or atypical lymphocytes are present, stage 5 (bone marrow involvement) is likely. The prognosis is then worse. Also important are the clinical substages a) clinically good general condition and b) clinically ill (e.g. vomiting, PU/PD, weight loss). The prognosis is significantly better in substage a). Prof Dr Rohrer Bley points out that the situation in cats with nasal lymphoma is somewhat different. Nasal lymphoma is a localised disease that can be treated with radiotherapy. Any systemic involvement should be excluded beforehand through thorough staging (thoracic radiographs, ultrasound of kidneys and abdominal lymph nodes, cytology of altered lymph nodes as well as of liver and spleen).
Dr Karpenstein-Klumpp can provide reassurance regarding ultrasound-guided punctures of internal organs. It is not that difficult. The spleen in particular is easy to reach. The sewing needle technique (forwards and backwards, not fanning) without aspiration is ideal. In many patients, the puncture is successful without complications, even without sedation. However, this should be decided after individual assessment of the patient, personal expertise, and the organ to be punctured.
The therapy depends on the type of lymphoma. The primary treatment is medication. Some types of lymphoma, such as nasal lymphoma in cats, can be effectively treated by radiotherapy (if they are actually confined to the nasal cavity). Surgical options are limited. Surgery can be used for singular skin nodules, individually affected lymph nodes, and to remove an ileus in intestinal lymphoma, but is always accompanied by drug therapy. In the case of feline renal lymphoma in particular, it is important to bear in mind that this is a bilateral disease.
The unilateral removal of one kidney is pointless.
Dr Schmidt advises that pet owners should be thoroughly informed about the side effects and risks, but without creating unnecessary fear.
As the term “chemotherapy” often leads to false associations, he prefers to speak of “drug-based cancer therapy”. As a rule of thumb, he gives the following prognosis for large-cell, multicentric lymphoma in dogs undergoing chemotherapy: 50% of dogs with B-cell lymphoma are still alive after 12 months, and in the case of T-cell lymphoma, after 7–8 months. It is important to note that these are statistical values. In individual cases, long survival times can be achieved — in some instances, even several years. A cure is possible, but rare. The use of glucocorticoids alone is considered palliative, and half of the dogs die within 2–3 months.
A complete chemotherapy cycle usually lasts 4–5 months. Most protocols include doxorubicin, vincristine, cyclophosphamide and prednisolone — the so-called CHOP protocol. For T-cell lymphomas, a protocol containing lomustine is often preferred (commonly referred to as LOPP). In cats, vincristine, cyclophosphamide and prednisolone (COP) are often used alone. The active substances are selected so that drug classes with different mechanisms of action alternate, in order to achieve the broadest possible therapeutic spectrum. Doxorubicin and vincristine must be administered intravenously, whereas cyclophosphamide, lomustine and prednisolone are available as oral medications. A purely oral “tablet-based” chemotherapy is generally less effective, as it lacks key agents such as doxorubicin and vincristine. An exception to this is small-cell intestinal lymphoma in cats.
Possible side effects include loss of appetite, vomiting, diarrhoea, and secondary infections as a result of immunosuppression (chemotherapy-induced leucopenia). Local tissue damage may also occur around the venous access site if the chemotherapeutic agent is not administered correctly. A particular concern with doxorubicin is its potential cardiotoxicity; it should not be used in patients with pre-existing cardiac conditions.
Moreover, several chemotherapeutic agents — including vincristine and doxorubicin — are con- traindicated in patients with an MDR1 gene defect.
When handling chemotherapeutic agents, the safety of the personnel involved must be ensured. These drugs should only be prepared under a specialised fume hood. Alternatively, they can be ordered from selected pharmacies that supply them in a closed system. It is crucial to provide thorough instruction on the proper handling of chemotherapeutics for both veterinary staff and pet owners. The substances can be excreted in urine, faeces, and saliva. However, it remains unclear to what extent this poses a health risk to humans or animals in contact with treated pets. Particular caution should be taken with pregnant individuals and young children. Blood samples collected shortly after chemotherapy should also be handled with care.
Dr Rohrer Bley notes that one of the distinct features of lymphoma is its radiosensitivity. Due to the typically widespread nature of the disease and/or intrathoracic or intra-abdominal localisation, radiotherapy is often not a practical option.
However, excellent results can be achieved in cases of feline nasal lymphoma. A standard protocol includes 10 sessions of radiation over two weeks.
Clinical improvement is typically rapid, with median survival times of 2–3 years. Nevertheless, systemic progression can occur later in about one-third of patients.
Radiotherapy may also be used in cases of cutaneous lymphoma, provided the solitary skin lesions are detected early, before widespread dissemination occurs, or if the disease remains confined to the oral cavity.
With regard to monitoring, Prof. Dr Rohrer Bley reports that she generally refrains from regular follow-ups. Instead, she educates clients on recognising clinical symptoms, so that patients can be presented promptly in the event of disease progression. Dr Schmidt recommends regular weighing of cats, advising owners to seek veterinary examination in cases of significant weight loss.
Dr Karpenstein-Klumpp highlights the importance of accommodating the wishes of pet owners — many prefer regular veterinary visits, and some request ultrasound examinations. Dr Schmidt confirms that owners often express a desire for routine check-ups. Dr Lapsina adds that smaller (e.g. hyperglobulinaemia, hypercalcaemia, LDH) and larger tumour markers (e.g. thymidine kinase) may also prove useful in monitoring disease progression.
Dr. Jennifer von Luckner