A body cavity effusion is defined as the accumulation of fluid in a body cavity, such as the thorax, abdomen, or pericardium. Animals with body cavity effusions present relatively frequently in clinical practice. Clinical signs may include dyspnoea, cardiac arrhythmias, limited auscultation of the heart, and an enlarged, often painful abdomen.
A wide range of diseases can be responsible. In addition to inflammation and infection, neoplasms or other space-occupying processes, as well as trauma, metabolic disorders, or cardiovascular diseases, may lead to the development of a body cavity effusion. For diagnostic evaluation, analysis of the effusion is therefore essential. Parameters assessed include macroscopic appearance, the proportion of different cell populations, physicochemical tests (e.g., total protein, albumin, triglycerides, bilirubin, Rivalta test), and cytological examination of the cells.
Sample Preparation
As a general rule, effusions should always be collected into two separate tubes. One tube should be an EDTA tube to prevent clotting of the sample.
In addition, a plain tube (e.g., an uncoated serum tube) should be filled. From the EDTA tube, the total nucleated cell count (TNCC) is measured, the erythrocyte content (PCV, haematocrit) is determined in cases of blood admixture, and smears are prepared for cytological examination.
The plain tube is used to determine clinical-chemical and physicochemical parameters. It is important that this tube is centrifuged promptly and that only the supernatant is used, in order to avoid skewing the results. For example, glucose concentration decreases over time depending on the cell count, as glucose is consumed by the cells or bacteria.
Bacteriological analysis can be performed either from the fluid in the plain tube or by taking a swab with medium from this tube. In any case, bacteriological testing can not be performed from the EDTA tube, as the EDTA coating has bactericidal effects.
-
-
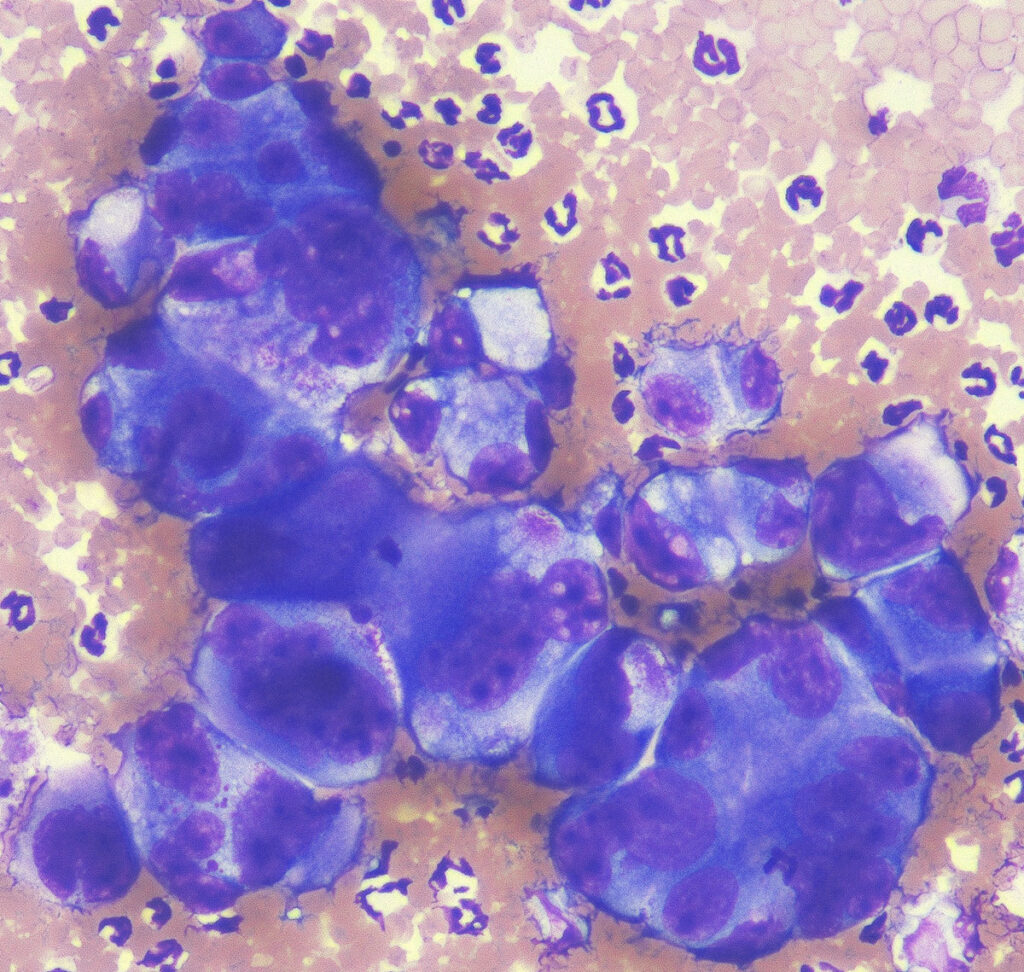
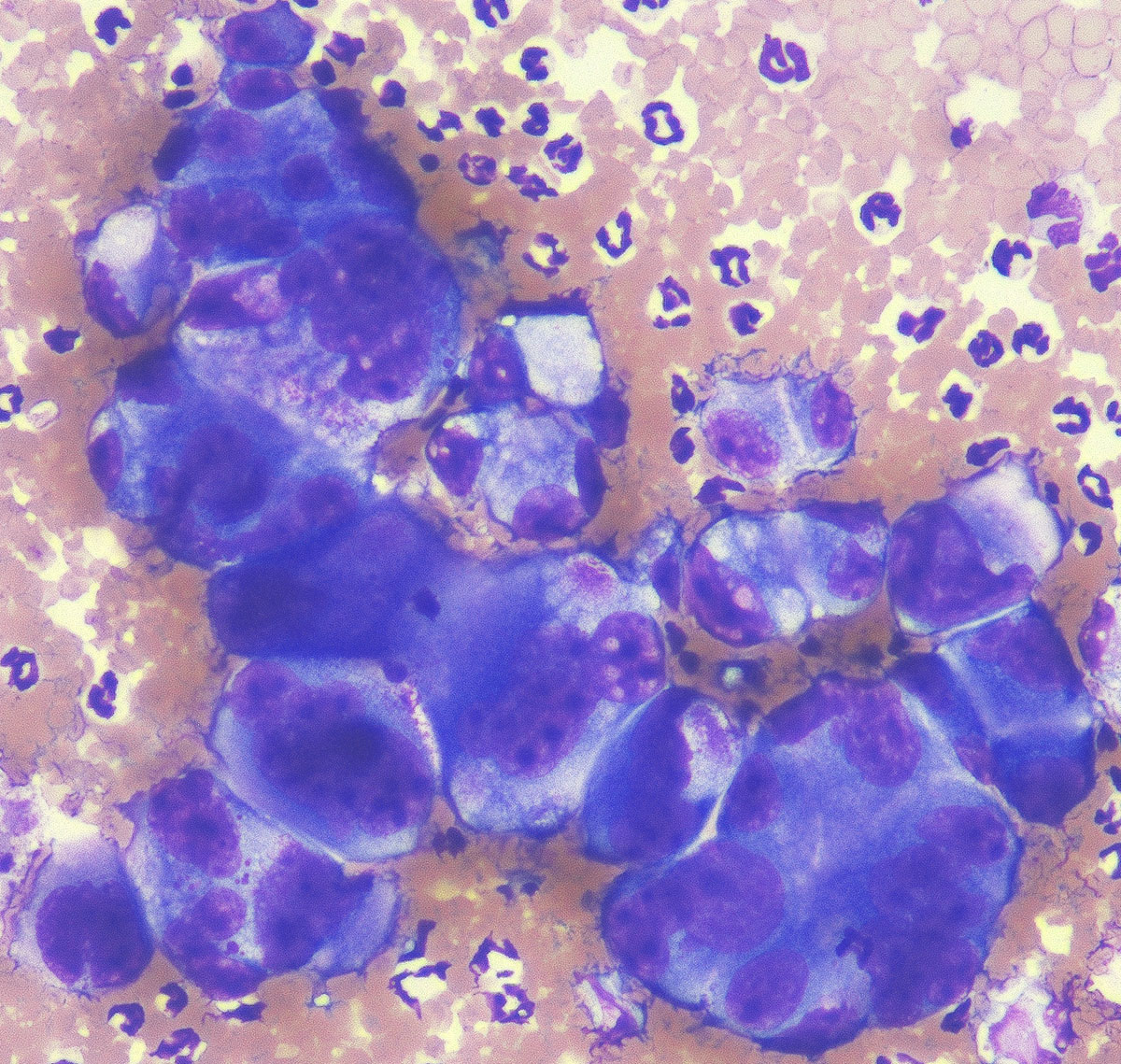
Fig. 1A: Pleomorphic cells of a carcinoma
Picture credits: Laboklin
-
-
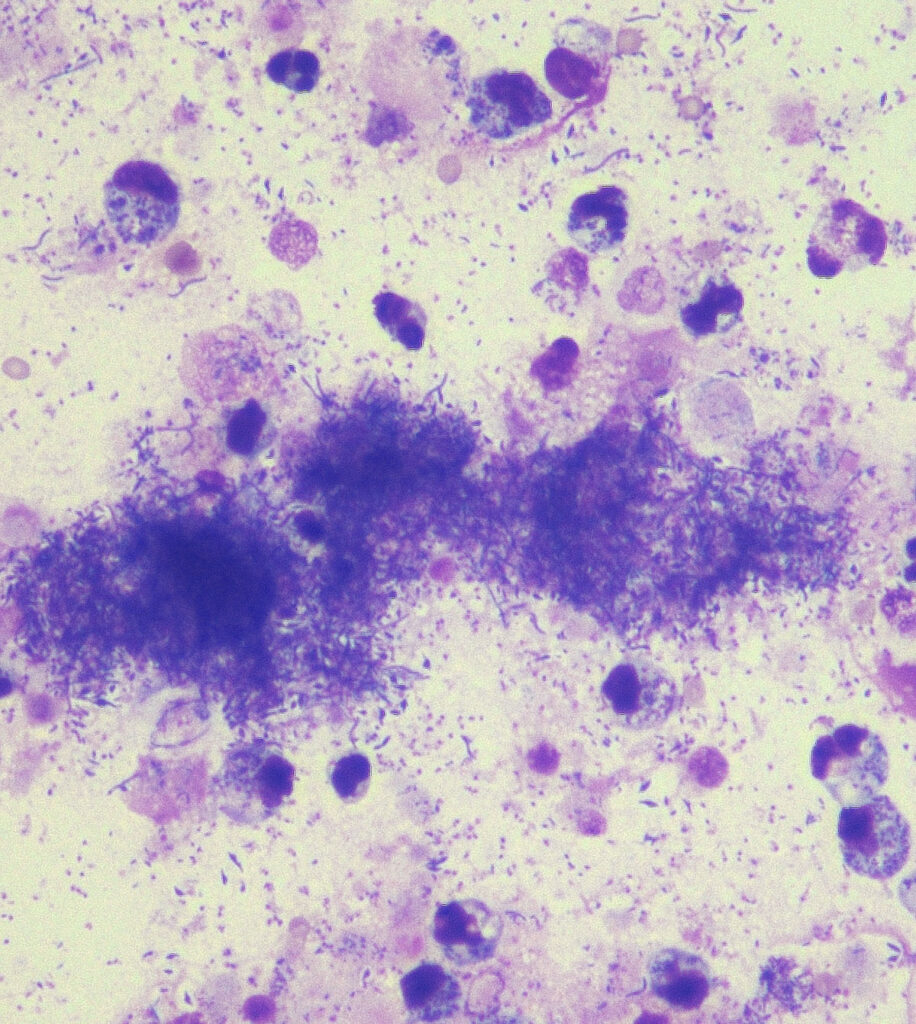
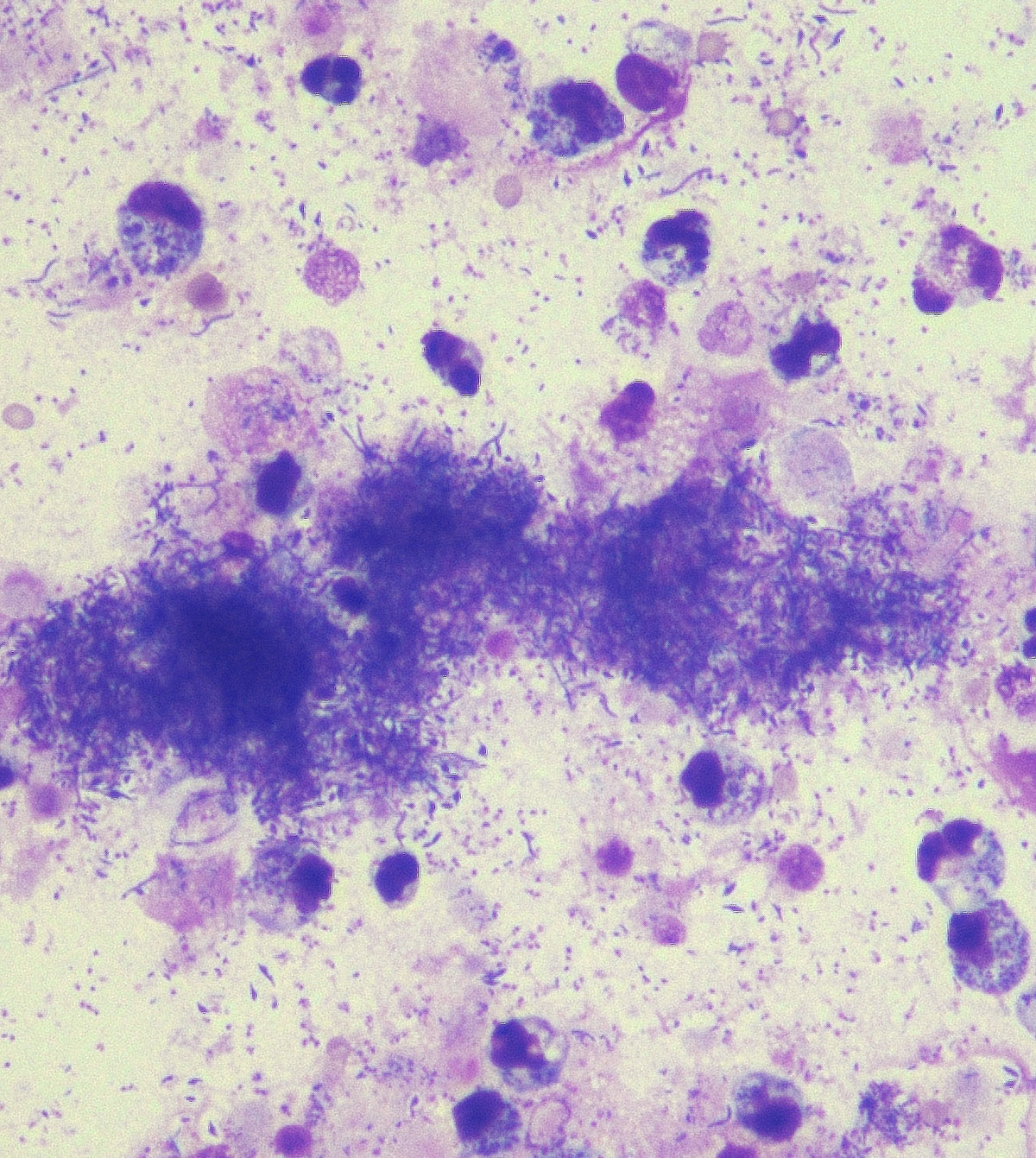
Fig. 1B: septic effusion; Diff-Quick stain, 400× magnification
Picture credits: Laboklin
For cytological examination, a smear should always be prepared directly in the clinic to ensure optimal cell preservation. Depending on the type of effusion, either a direct smear is sufficient (for cell-rich or blood-rich effusions; prepare the smear similarly to a blood smear) or cell concentration is required (for cell-poor effusions; smear with a stop line, sediment smear, or cytocentrifuged preparation).
For an external laboratory, it is essential to indicate whether a cell concentration was performed.
Only with this information can the cell count be accurately assessed, allowing correct classification of the effusion. A cell-rich direct smear has a different significance (e.g., exudate) than a cell-rich centrifugate (which may indicate a transudate). If samples are being prepared for shipment to an external laboratory, it is also important to include the preliminary report.
Relevant information are the signalment, clinical course, previous diagnostics, prior treatments, and the macroscopic appearance of the effusion if the fluid itself is not being sent.
Effusion Analysis – Macroscopic Findings
The assessment of colour and turbidity of the effusion can already provide useful informations (Table 1). However, the underlying cause of the effusion is generally not identifiable macroscopically.
Table 1: Broad classification of effusions based on macroscopic appearance
| Diagnosis | Colour | Consistency |
| Hydrothorax / hydroabdomen / hydropericardium |
clear | watery |
| Haemothorax / haemabdomen / haemopericardium | red | watery or coagulated |
| Serous inflammation | clear | watery, gelatinous |
| Fibrinous inflammation / chylous effusion | milky | watery, with flakes |
| Purulent inflammation | brownish | watery, creamy |
It is particularly important that macroscopic assessment is performed immediately at the time of collection. In cases of blood admixture, an iatrogenic process is more likely if initially clear fluid is aspirated that later becomes reddish. In contrast, with haemorrhagic effusions, the fluid is red from the beginning.
Basic Parameters
The initial classification of effusions is based on protein concentration and cell count (Table 2).
If total protein measurement is not possible in the clinic, specific gravity can alternatively be determined using a refractometer. The total nucleated cell count (TNCC) can be measured either automatically using a haematology analyser with appropriate settings or manually using a haemocytometer. A semi-quantitative estimate is also possible from a smear during cytological examination (cell count per field × objective² = cells/ml). In specific cases, automated measurement should be avoided, for example, when a septic effusion is suspected (risk of contamination) or when the effusion is highly viscous or flocculent (risk of clotting). Using these parameters, effusions are classified as low-protein transudates, high-protein transudates, or exudates. In veterinary medicine, the term “modified transudate” is commonly used as a synonym for high-protein transudate. However, as it generally does not represent a modification during effusion formation, this term is increasingly avoided in more recent literature.
Table 2: Basic classification of effusions based on clinical-chemical parameters
| Cell Count (µl) | Protein (g/l) | Specific Gravity (g/l) | |
| Low-protein transudate | < 1.500 | < 25 | < 1018 |
| High-protein transudate | 1.000–7.000 | 25–75 | 1018–1025 |
| Exudate | > 5.000 | > 30 | > 1025 |
The classification described above is, however, very general and cannot reflect the full range of effusions and their underlying pathogenesis.
Further testing is often required. To differentiate between transudates and exudates, the simplified Light’s criteria can also be applied. An effusion is considered an exudate if the lactate dehydrogenase (LDH) concentration in the fluid exceeds two-thirds of the upper reference interval and the total protein in serum is greater than 4.0 g/dl. Classification using C-reactive protein (CRP, a major acute-phase protein) has also been described. The cut-off value in this case is 4 μg/ml. If this value is exceeded, the effusion is considered an exudate.
Specialised Investigations
For specific effusions, additional parameters are available (Table 3). In the case of a blood-rich, it is important to determine whether the blood was introduced iatrogenically during sampling or is originally present in the effusion. A haematocrit value of >3 % is considered indicative of a significant blood component.
The effusion haematocrit should be compared with the current peripheral blood haematocrit.
Haemorrhagic effusions can occur, for example, due to trauma, ruptured tumours (such as haemangiosarcoma), or coagulopathies (e.g., rodenticide poisoning).
For septic effusions, glucose and lactate can be assessed. Both parameters must be measured promptly after sample collection to avoid distortion of results. Glucose decreases due to consumption by cells or bacteria, while lactate increases as a product of anaerobic glycolysis. The differences between serum and effusion values are then calculated. Findings above the corresponding cut-offs (>20 mg/dl glucose, < -2 mmol/l lactate) suggest a septic effusion. Likewise, a lactate concentration >2.5 mmol/l is indicative of a septic process. However, neither parameter is specific, and the suspicion should be confirmed with additional tests. Bacteriological examination is also recommended in such cases.
For lymphocyte-rich effusions, triglyceride and cholesterol concentrations can help determine whether a chylous effusion is present. It is best to compare triglyceride concentrations in the effusion and serum (chylous effusion: effusion triglycerides > serum). Very high triglyceride concentrations in the effusion (>100 mg/dl) and a low effusion cholesterol/triglyceride ratio (<1) are also indicative of chylous effusions. It should be noted that lymphocyte-rich effusions are most commonly caused by heart disease (~70 %) rather than neoplasia (~25 %).
If a lymphoma is suspected, lymphocyte clonality can be assessed using PARR or immunophenotyping can be performed by flow cytometry. PARR is well suited to confirm lympho-ma, but a negative result does not rule it out; only a positive result is diagnostic. Immunophenotyping requires good cell preservation, so the sample must not be too old (see also LABOKLIN Aktuell, Issue 11/2024: “Leukaemias in Dogs and Cats”).
Thymidine kinase is a proliferation marker and can provide valuable information, particularly during follow-up, although it has not yet been validated for pleural effusions.
If an uroperitoneum is suspected, creatinine and potassium can be measured and compared in effusion and serum. In cases of suspected bilious effusion, bilirubin can be assessed accordingly.
If pancreatitis is suspected, lipase can be measured in the effusion (Table 3).
In cases of suspected feline infectious peritonitis (FIP), tests in addition to elevated total protein (>45 g/l) include the albumin/globulin ratio (<0.6) and the Rivalta test (positive). Ultimately, detection of the pathogen is recommended, which can be performed using coronavirus PCR from the effusion.
Table 3: Parameters for specific diagnostic questions
| Parameter | Cut-off / Result | |
| Haemorrhagic effusion | Haematocrit / PCV | effusion > serum, > 3 % significant |
| Septic effusion | Glucose
Lactate |
serum – effusion = > 20 mg/dl Serum – Erguss = |
| Chylous effusion | Triglycerides
Cholesterol |
triglycerides > 100 mg/dl or effusion > serum (3:1) or cholesterol/triglyceride ratio < 1 |
| Lymphoma | Lymphocyte clonality (PARR)
Flow cytometry
Thymidinkinase |
monoclonal proliferation
predominance of a lymphocyte subpopulation (surface markers) proliferation marker |
| Uroperitoneum | Creatinine Potassium | effusion > serum (2:1) effusion > serum (1,4:1) |
| Bilious effusion | Bilirubin | effusion > serum (2:1) |
| Pancreatitis | Lipase | effusion > serum |
| FIP | Albumin, Globulin
Rivalta test Coronavirus-PCR |
A/G ratoio < 0,6
Rivalta test positive coronavirus-PCR from effusion or corresponding lesions (tissue) positive |
Cytology
Semi-quantitatively, cytology itself can provide a rough estimate of cell count and protein content, allowing a preliminary classification of the effusion type. However, automated measurements are generally preferred. The main question addressed by cytology is usually which cells are present. In particular, cytology is used to search for tumour cells or intracellular microorganisms. It also allows microscopic differentiation of leukocytes (e.g., increased neutrophils or eosinophils, lymphocytes, macrophages).
If a septic effusion is suspected, cytology is advantageous for several reasons: to estimate the cell count (these samples should not be measured in automated analysers due to contamination or clotting risk), to detect intracellular pathogens (differentiation from secondary contamination), and to assess the morphology of neutrophils (degenerative changes). Cytological detection of filamentous bacteria (e.g., Nocardia spp., Actinomyces spp.) can also be diagnostically significant, as these bacteria require special culture requirements. Additinally, cytology can sometimes provide information on chronicity. For example, in haemorrhagic effusions, erythrophagocytosis can be observed within a few hours, whereas siderophages typically appear after approximately 2–4 days. Both are indicators of red blood cell breakdown. The presence of platelets without signs of red cell degradation suggests an iatrogenic or peracute process.
Certain cytological structures can further indicate the origin of the effusion. In an uroperitoneum, urine crystals may be present; in a bilious effusion, bilirubin crystals or bile can be detected.
Mesothelial cells may be present in any effusion. In chronic effusions / chronic inflammation, these cells can exhibit marked dysplasia, which makes a morphological differentiation of mesothelial and carcinoma cells challenging or in some cases impossible. In neoplastic effusions, it is important to note that the primary tumour does not necessarily reside in the same compartment. Moreover, only a positive cytology result is definitive, as not all neoplasms shed tumour cells into the effusion.
Conclusion
With only a few parameters (macroscopic findings, total protein, and cell count), it is generally possible to perform a rough classification of the effusion already and thus narrow down the differential diagnoses. However, additional investigations are often required depending on the suspected diagnosis. This article summarises the most commonly used parameters (see Tables 1–3). Cytological examination provides further specific information and is particularly important for septic and neoplastic effusions. It can also provide valuable information in cases of hemorrhagic effusions, uroperitoneum, and bilious effusions.
If only a small volume of material can be obtained, cytology is always recommended, as it allows at least a semi-quantitative basic classification in addition to the morphological assessment.
Dr. Katrin Törner
Our Services on This Topic
- Cytology / Cytology Requiring Increased Effort
- Body Cavity Effusion Analysis (Cytology, total protein, cell count, Rivalta test [cat], cholesterol, triglycerides, albumin/globulin ratio)
- Body Cavity Effusion FIP Cat (Cytology, total protein, cell count, Rivalta test, albumin/globu-lin ratio, coronavirus PCR)