Giardia (G.) intestinalis (syn. G. duodenalis, G. lamblia) occurs in a wide range of vertebrates. In animals under one year of age, Giardia is one of the most common endoparasites. Cysts are excreted not only by animals with clinical symptoms, such as small intestinal diarrhoea, but also by those with inapparent infections. Infection induces partial immunity, which is why the detection rate in animals older than one year decreases significantly. However, reinfections can still occur despite this partial immunity.
Giardia are flagellated protozoa that cannot be morphologically distinguished from other protozoa under the microscope. Host specificity has always been considered minimal, though very few Giardia strains isolated from small animals cause disease in humans.
Types
Several genotypes (assemblages) with distinct host specificities are recognised (A-G). Assemblage A (G. duodenalis) occurs primarily in humans and various other mammals but is rarely found in dogs and cats. Assemblage B (G. enterica) is also mainly detected in humans and only occasionally in dogs and cats. Assemblages C and D (G. canis) are associated with infections in dogs, while assemblage F (G. felis) is specific to cats.
Genotyping of the different Giardia assemblages can be carried out via PCR following a positive result. Transmission of human-pathogenic Giardia assemblages from dogs to humans is considered unlikely under normal hygienic conditions.
Life Cycle
Giardia cysts are ingested orally and excyst into trophozoites in the small intestine. These trophozoites attach to the mucosal epithelial cells of the small intestine, where they multiply through repeated binary fission and subsequently form new cysts. The prepatent period ranges from 4 to 16 days.
The cysts are highly resistant and immediately infectious, and are intermittently shed in large quantities via the faeces into the environment over a period of weeks to months (patency).
They remain infectious in moist environments for at least three months and in faeces for around one week. However, they are sensitive to dehydration and cold temperatures (e.g. −4 °C for over one week).
Transmission occurs via the oral route as a dirt- or smear-borne infection, as well as through faecally contaminated water and feed. The minimum infectious dose is very low, requiring only a few cysts.
Clinical Manifestations
In addition to inapparent courses, Giardia can cause chronic intermittent diarrhoea with a thin, mushy to watery consistency and mucus, as well as vomiting, weight loss, and apathy. Destruction of the glycocalyx and adhesion to the microvilli leads to malabsorption. Enzymes are inhibited, and an inflammatory reaction follows.
Several methods are available for diagnosing a Giardia infection.
Diagnosis
Microscopy
Native preparation
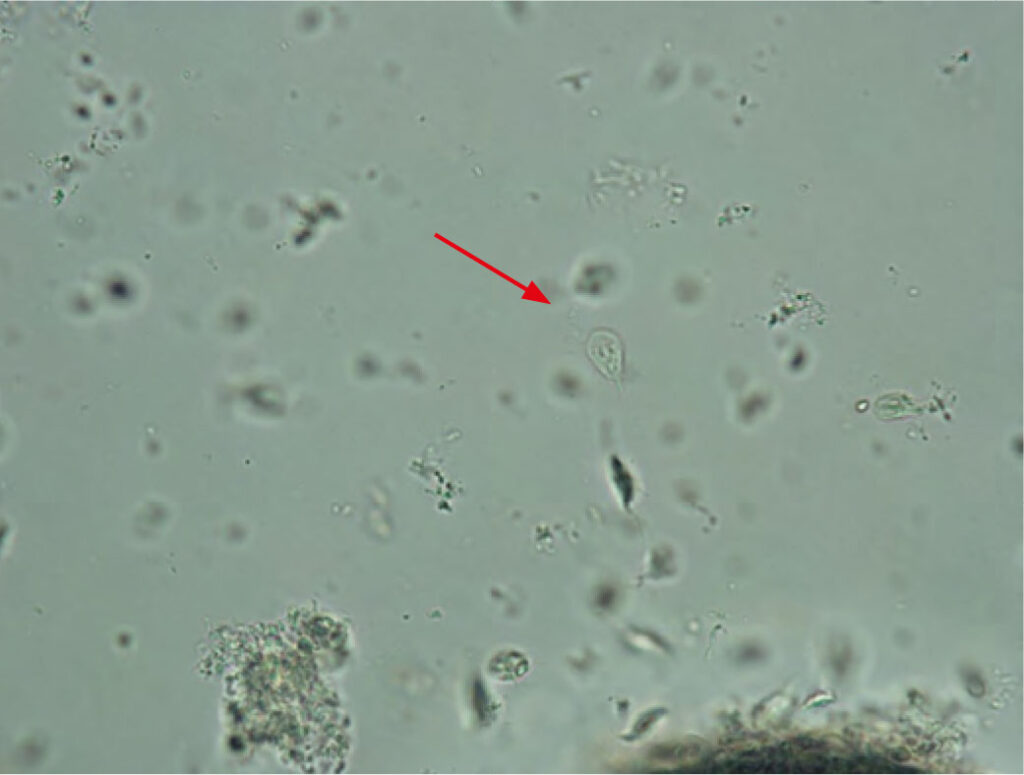
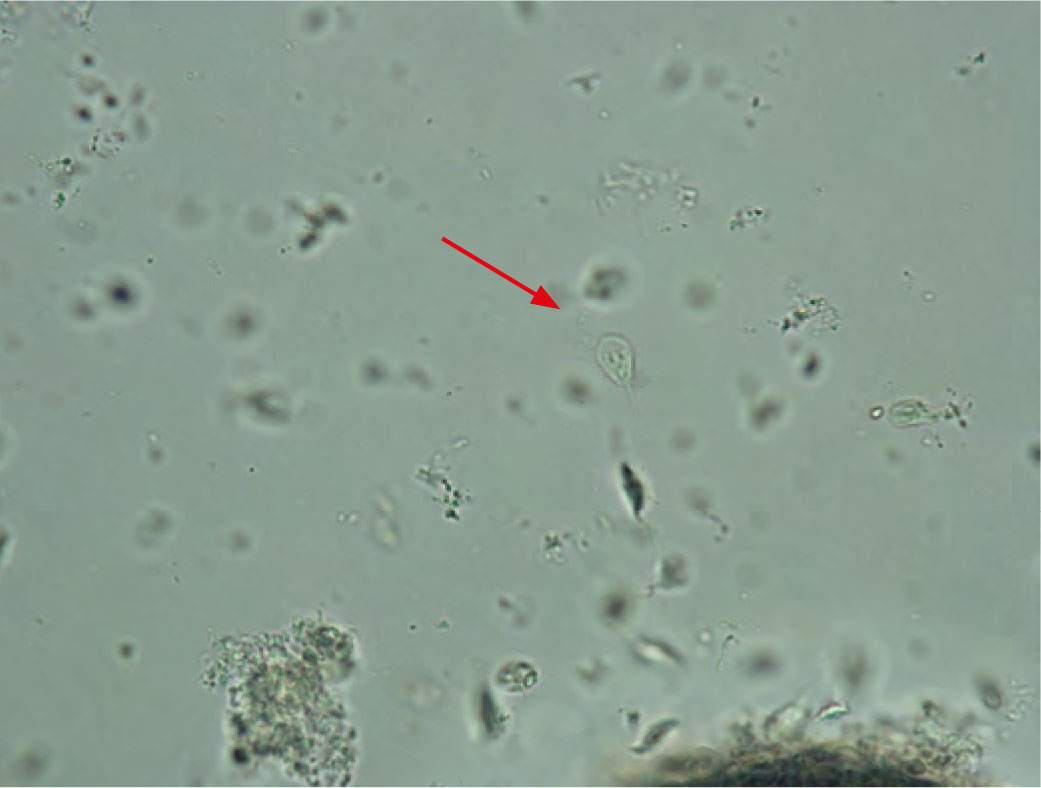
Trophozoites can be detected in fresh faeces immediately after defecation. To do this, a pea-sized amount of faeces is mixed with a small amount of physiological saline solution, transferred to a microscope slide, and covered with a cover slip. The typical trophozoites are then visible under a microscope in their native state (Fig. 1).
At this stage, Tritrichomonas foetus can also be identified in cats (400x magnification). The different movement patterns can be used to differentiate between Giardia (‘falling leaf’) and Trichomonads (e.g. Tritrichomonas foetus twitching and rotating, tending to remain in one place).
-
-
Fig. 1: Giardia trophozoite (400x magnification)
Image source: Laboklin
-
-
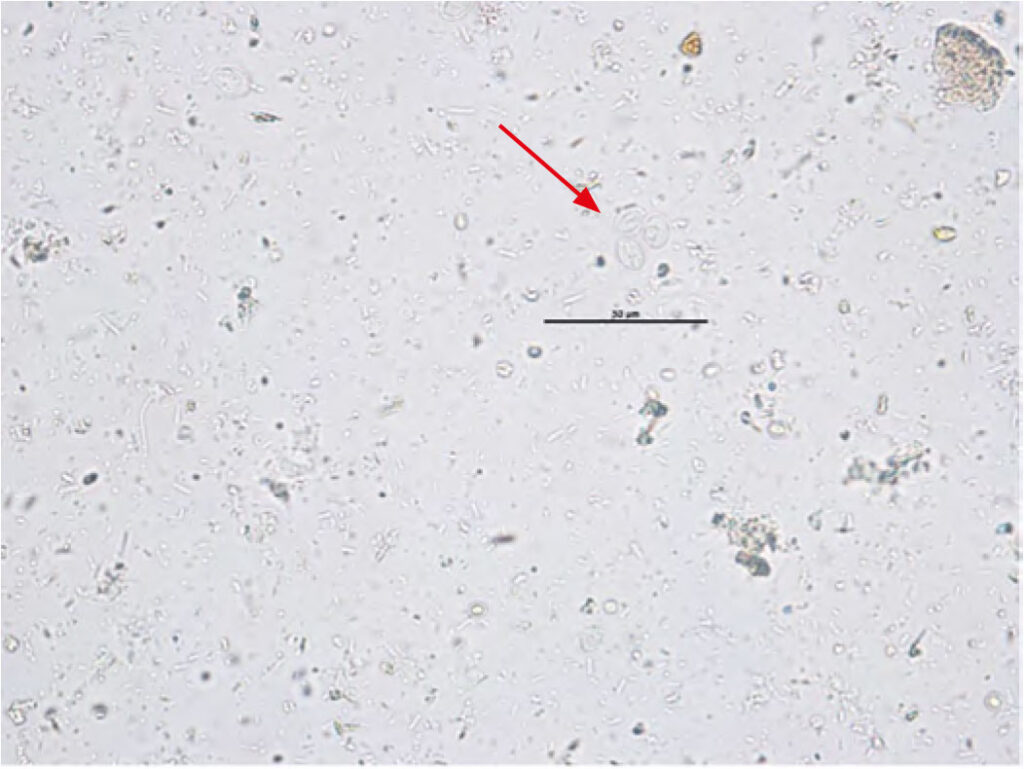
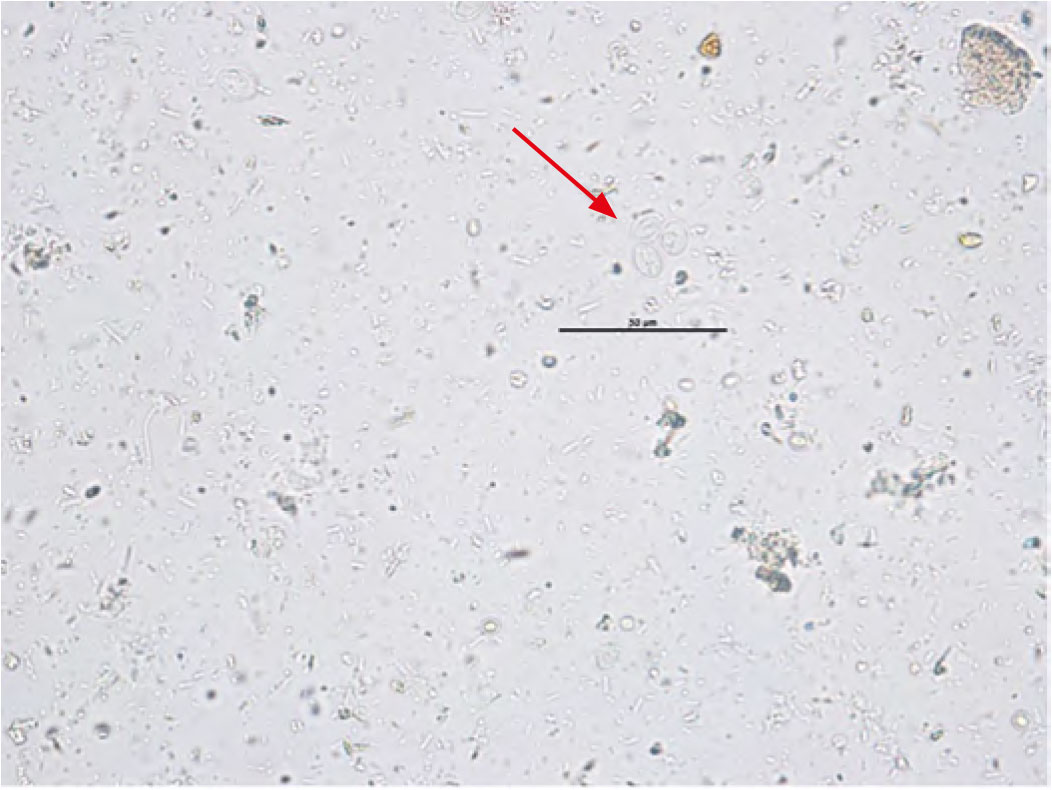
Fig. 2: Giardia cysts (400x magnification)
Image source: Laboklin
-
-
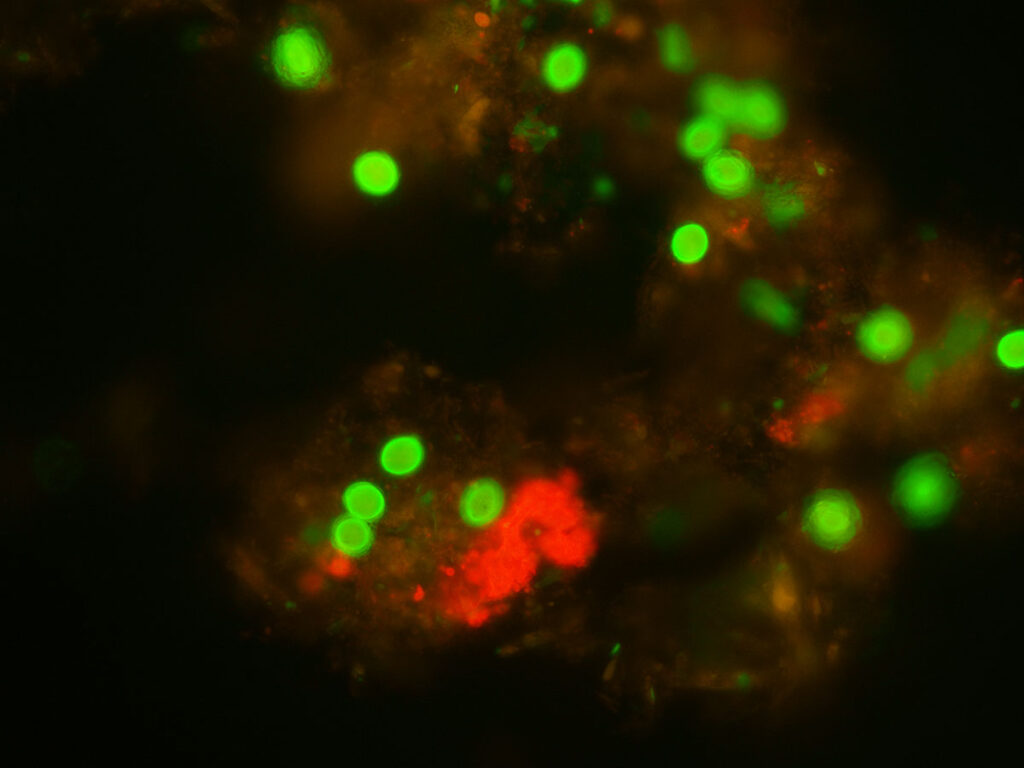
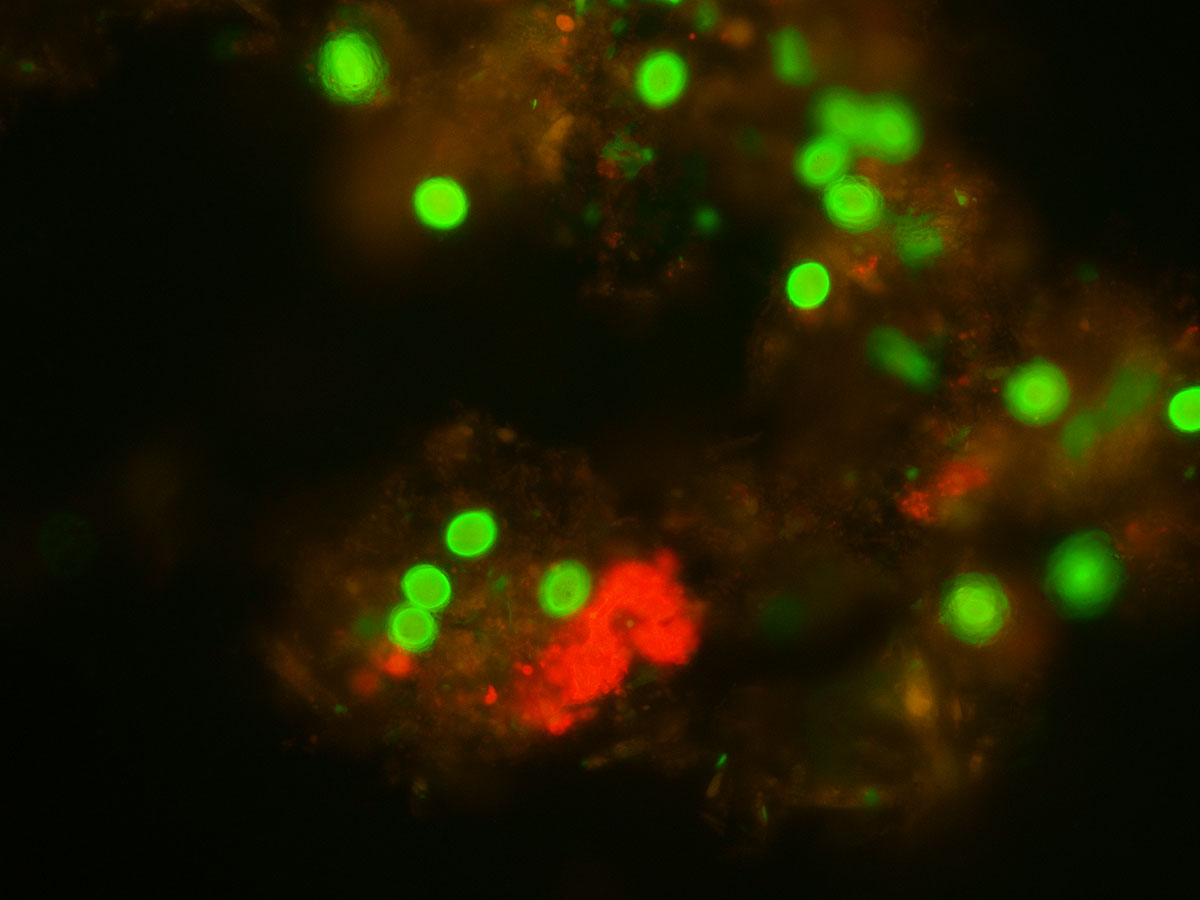
Fig. 3: Cysts (green) under a fluorescence microscope (400x magnification)
Image source: Laboklin
-
-
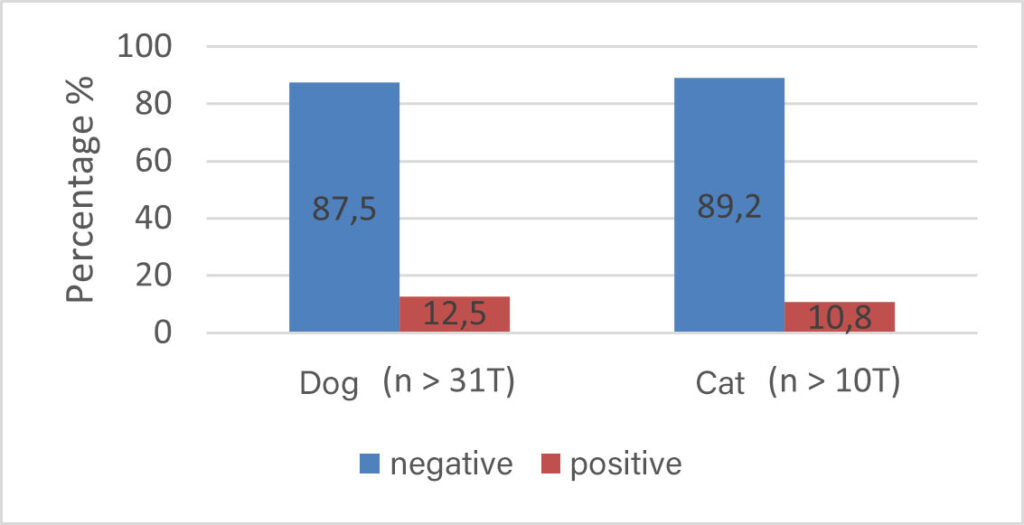
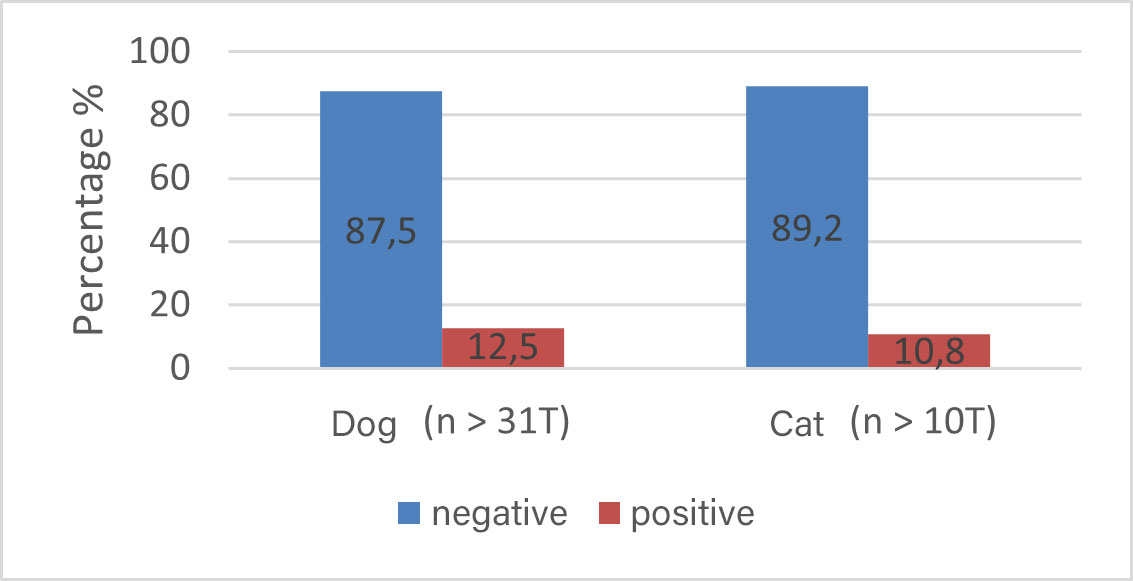
Fig. 4: Detection rates using EIA
Image source: Laboklin
-

-
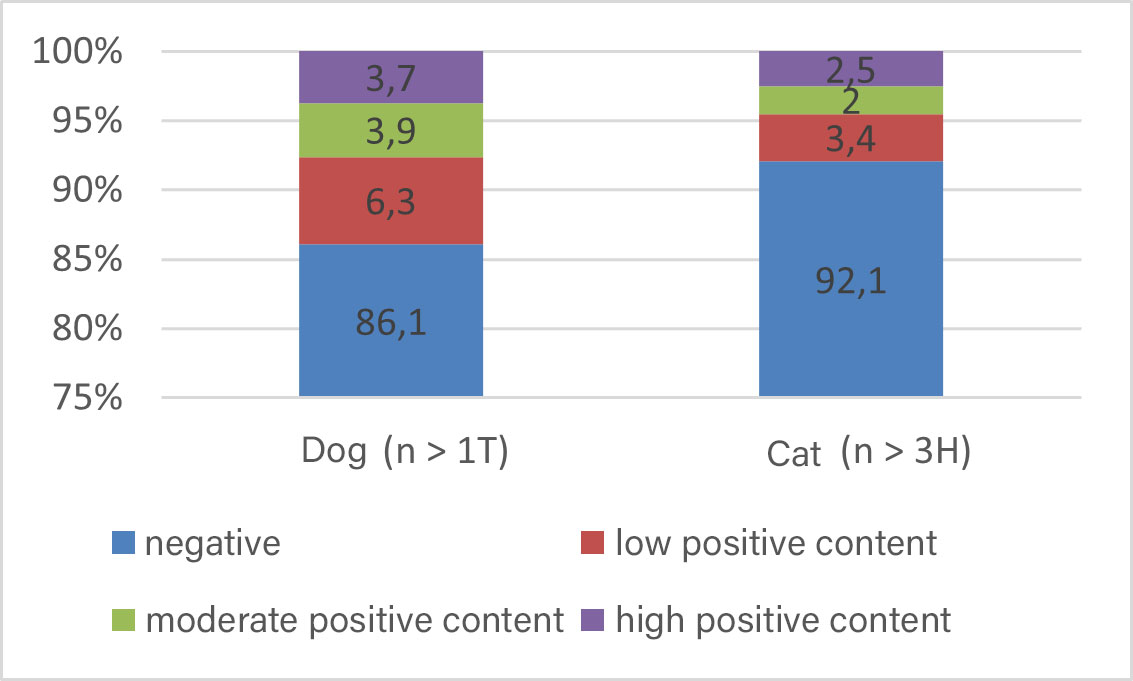
Fig. 5: Detection rates using IFAT
Image source: Laboklin
-

-
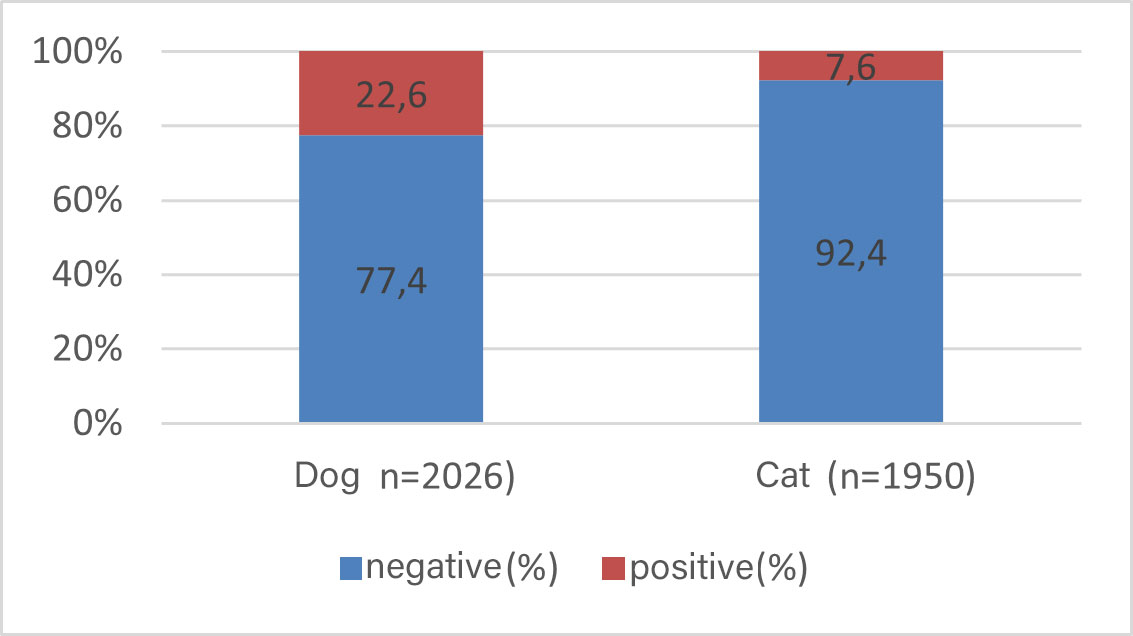
Fig. 6: Detection rates using PCR
Image source: Laboklin
Flotation / Sedimentation
In flotation, the cysts are severely damaged by the high salt content of the flotation solution. A more suitable method is enrichment using SAFC (sodium acetate-acetic acid-formalin concentration), a specialised sedimentation process. To increase the sensitivity of this microscopic detection method, a stool sample should be collected over 2–3 days, as cyst excretion varies greatly in intensity and is intermittent. In the SAFC enrichment method, the typical cysts appear with a thin shell and an axial rod. They are usually easily recognisable at 400x magnification (Fig. 2).
There is a risk of confusion, particularly with yeasts, which may have a similar shape and size but, unlike Giardia, lack nuclei or median bodies. Microscopy is less sensitive than immunological detection. This should be taken into account when selecting the diagnostic method.
Immunological Methods
IFAT (Indirect Fluorescence Antibody Test)
The cysts excreted and enriched using the SAFC method can be stained using a fluorescence technique and then more easily detected under a microscope using special light filters (Fig. 3).
EIA (Enzyme-Linked Immunosorbent Assay)
The two main proteins of the cyst wall (Cyst-Wall-Proteins) CWP-1 and CWP-2 combine to form a large heterodimer, the so-called Giardia-specific antigen, GSA-65. This is then detected using an enzyme immunoassay (EIA). Due to enzyme amplification of the colour reaction, EIA has higher sensitivity and, due to the washing step, higher specificity compared to non-enzyme immunoassays (NEIAs), such as those used in rapid tests in practice. The available copro-antigen tests can therefore differ in their results, but are overall significantly more sensitive than microscopic detection of Giardia cysts. This means that even in cases of temporary cessation of cyst excretion, a diagnosis can be made using a stool sample. The sensitivity and specificity of these ELISAs are approximately 98%.
PCR
Here, molecular biological detection of Giardiaspecific DNA from enriched cysts is performed using PCR or direct copro-PCR. The sensitivity is similar to that of detection using ELISA. Inhibitors in faeces can lead to false-negative results. PCR is particularly useful in positive samples for differentiating between different assemblages to exclude human pathogenic strains in a positive animal.
Results of Different Detection Methods
EIA
Giardia-specific antigen was detected in 12.5% of dog samples and 10.8% of cat samples using EIA (Fig. 4).
IFAT
The detection rate using immunofluorescence after enrichment using SAFC was 14% in dogs and 7.9% in cats. Here, it was also possible to indicate the quantity of cysts semi-quantitatively (Fig. 5).
PCR
The detection rate of Giardia-positive samples using PCR was 22.6% in dogs and 7.6% in cats (Fig. 6).
Evaluation
The selection of the appropriate test method depends on several factors. If clinical symptoms such as diarrhoea and vomiting are present, parasitological examination by flotation and Giardia detection by EIA are always recommended as the first step, using a pooled faecal sample. Among these, EIA is more sensitive than flotation. Antigen detection by IFAT is also possible. If differentiation of Giardia assemblages is required, PCR is the method of choice. If the parasitological result is negative, further diagnostic investigations should be undertaken to clarify the cause of the symptoms.
Even after successful treatment, EIA results may remain positive, as the method also detects non-viable (dead) Giardia. The same applies to PCR, which is even more sensitive and can detect DNA for several days post-treatment.
The excretion of infectious cysts following successful therapy can be most reliably demonstrated by IFAT after enrichment using the SAFC method.
Treatment
According to the ESCCAP (European Scientific Counsel Companion Animal Parasites) guidelines, treatment of clinically asymptomatic Giardia carriers is generally not recommended. However, it is indicated in animals exhibiting gastrointestinal symptoms.
In Germany, veterinary medicinal products containing the active substances fenbendazole and metronidazole are authorised for the treatment of giardiasis in dogs and cats.
In addition to pharmacological treatment, consistent hygiene measures are essential to achieve sustained therapeutic success.
Fenbendazole
The recommended dosage for dogs and cats is 50 mg/kg body weight once daily for 3 to 5 days.
However, in practice, a treatment duration of 3 days is often insufficient. Therefore, a 5-day treatment is recommended from the outset.
Metronidazole
The recommended dose is 25 mg/kg body weight twice daily for 5 to 7 days. Due to the potential toxicity of metronidazole, this dose should not be exceeded — particularly in cats.
In practice, continued excretion of Giardia cysts and persistence of clinical symptoms are frequently observed despite treatment with these active substances. Treatment failure may be due to concurrent infections, reinfection from a contaminated environment, or incomplete elimination of the parasites.
Monitoring the Success of Treatment
According to ESCCAP, treatment should be monitored using one of the methods outlined above approximately 5 to 7 days after the completion of treatment. If the results remain positive and clinical symptoms persist, treatment should be repeated as necessary.
Dr. Anton Heusinger
Our Services Relating to Giardia
- Giardia EIA
- Giardia PCR
- Giardia IFAT
- Numerous profiles