Allergen-Specific Immunotherapy (ASIT, Hyposensitisation) is the only causal form of therapy for the treatment of canine atopic dermatitis (CAD). CAD is a chronic inflammatory skin disease in dogs caused by an allergic reaction to environmental allergens. The disease cannot be cured but can only be controlled and requires lifelong management.
ASIT is an effective and safe form of treatment. Successfully treated dogs show significantly reduced symptoms or may even become completely symptom-free. Numerous studies have demonstrated the success of the therapy in an average of two-thirds of the dogs treated. The administration of an extract containing the triggering allergens modulates the immunological reaction to environmental allergens.
The conventional protocol for ASIT consists of subcutaneous injections of the extract, which are administered initially at short intervals, then at prolonged intervals with increasing dosages, depending on the protocol, over a period of several weeks to months (initial treatment, initiation phase). The initial treatment is followed by subsequent treatments (maintenance phase), in which a constant amount of the extract is applied at longer intervals (usually 1 ml every 4 weeks).
According to the guidelines of the International Committee on Allergic Diseases of Animals (ICADA), it is recommended that ASIT be continued for at least 12 months before clinical success is assessed.
If a dog responds successfully to ASIT, it should be continued on a long-term or lifelong basis.
Questionnaire Study at Laboklin:
The aim of the study was to identify the reasons why ASIT was discontinued in dogs after the initiation phase (after the starter set) or during the maintenance phase (after at least one follow-up treatment). Dogs were selected from order lists for ASIT treatments at the Laboklin laboratory from 2020 to 2022, for which no further ASIT treatments were required. They were divided into two groups:
-
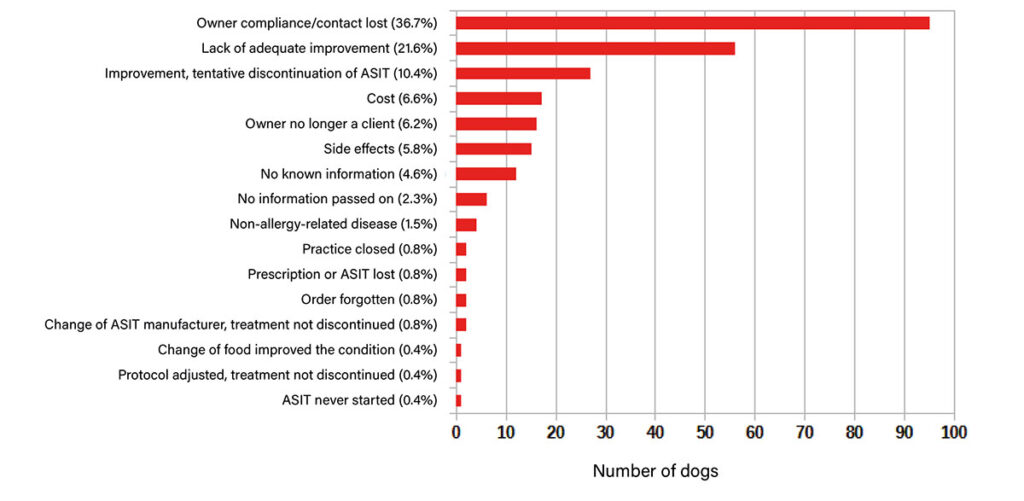
- Fig. 1: Reasons for discontinuation of allergen-specific immunotherapy (ASIT) in dogs after the starter set

-

- Fig. 2: Reasons for the discontinuation of Allergen-Specific Immunotherapy (ASIT) in dogs after at least one follow-up treatment

Group 1 (Discontinuation after the Starter Set): This group included dogs in which ASIT was discontinued after the initial treatment. Out of 2208 initial treatments, no follow-up treatments were ordered for 930 (42.1%).
Group 2 (Discontinuation after at least one follow-up treatment): This group included dogs in which ASIT was discontinued during the maintenance phase. In 1230 of 3662 ASIT follow-up treatments ordered (33.6%), no further follow-up treatments were ordered.
To determine the reasons for ASIT discontinuation, the treating veterinarians were contacted by telephone or via written questionnaires.
Several possible reasons could be selected by the veterinarians. The collected data was analysed descriptively and statistically.
Reasons for ASIT Discontinuation:
Cancellation after the starter set (group 1, fig. 1):
A total of 247 responses with 259 reasons for not receiving follow-up treatment after the initial treatment were analysed. Patients (n = 9) for whom no further ASIT was ordered due to death were not included in the analysis. The three most common reasons were lack of owner compliance/loss of contact (36.7%), insufficient/no improvement (21.6%), and discontinuation due to good treatment success (10.4%).
Cancellation after at least one follow-up treatment (Group 2, Fig. 2):
A total of 310 responses with 342 reasons given for why no further follow-up treatment took place were analysed. The average duration of ASIT treatment was 2.4 years. Patients (n = 42) for whom no further ASIT was ordered due to death were not included in the analysis. The three most common reasons for discontinuation of ASIT were lack of owner compliance/loss of contact (30.4%), insufficient/no improvement (23.7%), and discontinuation due to good treatment success (19%).
How Can ASIT Discontinuations Be Reduced and the Success of ASIT Treatment Optimised?
Initial treatments usually last for six months, which is significantly shorter than the recommended 12 months required to evaluate success. It can take up to a year for the maximum benefit of ASIT to become clinically apparent. In over 40% of the initial treatments in this Laboklin study, no follow-up treatments were ordered, and ASIT was therefore discontinued prematurely after the initial treatment.
If ASIT is successful after one year of therapy, it should be continued for life. Among the dogs examined during the maintenance phase, ASIT was discontinued in approximately 34% of cases.
Lack of owner compliance/loss of contact
The most common cause (about 37% in Group 1 and about 30% in Group 2) was a lack of owner compliance and/or a loss of contact between the veterinarian and the owner.
Owner compliance (Co-operation of the owner in implementing the recommended therapeutic measures) is a decisive factor for the success of the therapy. Owners should be educated in detail about the therapy protocol, the duration of therapy, the delayed onset of ASIT’s action, and the expected costs to optimise their expectations. A key factor here is continuous communication, especially during the first year of therapy.
In a study by Fennis et al. (2022), dogs that were regularly presented for veterinary check-ups in the first year of therapy showed a significantly higher success rate than those that were not monitored by a veterinarian. Regular check-ups not only ensure communication but also allow for continuous patient monitoring, enabling the diagnosis of secondary infections and adjustments to the protocol.
With accelerated and simplified initiation protocols (e.g., rush or cluster protocols and intralymphatic immunotherapy), the maintenance dose is reached more quickly. This approach could reduce the delay in effect and the time until success becomes clinically visible, thereby increasing owner compliance.
Another benefit of such initiation protocols is that ASIT injections are administered exclusively by the veterinarian, ensuring that patients remain under continuous veterinary supervision during the first months of therapy.
Less success than expected
The second most common reason for discontinuation in both groups was insufficient treatment success (approximately 22% in group 1 and approximately 24% in group 2). This was often mentioned in combination with poor owner compliance. The success of therapy should be assessed no earlier than after one year, which highlights an educational issue when ASIT is discontinued prematurely due to perceived lack of success after the initial treatment. These dogs were declared non-responders too early. The delayed onset of ASIT’s action should be clearly communicated by the veterinarian to manage owners’ expectations and reduce premature discontinuation within the first year of therapy, ultimately leading to higher ASIT success rates.
Anti-pruritic symptomatic therapies are often required during the initial months of ASIT to rapidly alleviate clinical signs until ASIT’s effects take hold. This is another factor that can improve owner compliance. However, the duration and dosage of such medications should be kept as low as possible. Pruritis should be reduced but not entirely eliminated, as completely suppressing pruritis can obscure the need for protocol adjustments.
Success rates of ASIT after at least one year of therapy are reported in the literature to be as high as 80% in dogs with CAD, aligning with the findings of this study (approximately 24% of cases in the maintenance phase were discontinued due to lack of success). It is generally expected that maximum treatment success will be apparent within the first year of therapy. If no clinical improvement is observed after one year and additional symptomatic therapies cannot be significantly reduced, the animal is classified as a non-responder, and ASIT is discontinued, as further response to therapy is unlikely.
Defining success correctly is crucial: ASIT is considered successful if the treated dogs exhibit more than a 50% improvement in clinical symptoms or if the need for additional symptomatic medication is reduced by more than 50%. CAD typically requires a multimodal treatment approach – a combination of several treatment options – to achieve optimal management.
In addition to consistent ectoparasitic prophylaxis, dogs experiencing acute allergic flare-ups should always be examined for secondary infections.
Acute flare-ups may necessitate short-term symptomatic therapies.
To further reduce the risk of ASIT failure, combination therapy should be considered, such as essential fatty acids, moisturising shampoos (to improve the skin barrier), and topical hydrocortisone products.
Before a dog is classified as a treatment failure, it should be carefully evaluated to determine whether there has truly been no improvement (e.g., using an itch scale, accurately recording the frequency of allergy flare-ups, and assessing the duration and dosage of additional symptomatic therapies).
Some respondents noted that ASIT was discontinued due to insufficient effectiveness, but that a deterioration in the condition occurred after discontinuation.
Another measure to optimise treatment success is the individual adaptation of the protocol, particularly with regard to the injection quantity and/or treatment intervals.
Furthermore, the lack of treatment efficacy in some patients could be explained by the presence of other pruritic conditions (e.g., food allergies or ectoparasites) that were not ruled out before starting ASIT. CAD is a diagnosis of exclusion, which should only be made after ruling out potential differential diagnoses and before initiating ASIT
Cancellation in case of successful response
The third most common reason for discontinuing ASIT in both groups was that the dogs had improved under treatment, leading to discontinuation of ASIT (approx. 10% in group 1 and 19% in group 2). Most patients require lifelong therapy to permanently manage CAD.
There is limited published data on the long-term effects of ASIT in dogs after therapy discontinuation. The few uncontrolled studies available indicate that most dogs deteriorate once ASIT is stopped.
This was also reported several times during the course of this study. Experience has shown that restarting ASIT can be complicated; allergy tests are often necessary, initial treatment must be restarted, and some dogs no longer respond as effectively.
It is therefore generally recommended not to interrupt ASIT if it is successful.
However, an individual attempt can be made to extend the injection intervals, as noted by 8.5% of respondents in group 2. If treatment success remains stable over several years during the maintenance phase, injection intervals can be gradually extended to up to 8 weeks.
Side effects
In approximately 6% of cases in group 1, ASIT was discontinued due to side effects.
The most common side effect of ASIT during the induction phase is increased pruritis after the injections, which also corresponds with the findings of the present study. If increased pruritis occurs immediately after the injection, the amount of allergen extract should be reduced, and the initiation protocol should be customised.
Owners should closely monitor their dogs’ reactions to the injections and provide immediate feedback to the treating veterinarian, so the ASIT protocol can be adjusted in the event of adverse reactions.
The Laboklin team is happy to assist with any questions regarding protocol adjustments.
Costs
In this study, costs were the reason for ASIT discontinuation in approximately 7% of group 1 and approximately 4% of group 2. For owners, the costs of ASIT in the first year, including the allergy test and regular veterinary check-ups, may appear high.
However, from an economic perspective, ASIT is much more cost-effective in the long term than purely symptomatic therapy. Poorly controlled allergy sufferers require more frequent veterinary visits, higher quantities of anti-pruritic medication, and more frequent treatment for secondary infections, as well as therapeutic measures for the potential side effects of symptomatic medication. This information can also help motivate owners to continue ASIT for the entire first year of treatment, or even into the second year of maintenance therapy, even if the therapy is moderately successful.
Conclusion
To summarise, ASIT is an essential component of the multimodal therapy management of CAD and a lifelong form of treatment that requires strong co-operation between owners and veterinarians.
The first year of therapy demands close monitoring of the patients and is the critical period for the success of the treatment.
The most common reasons for ASIT discontinuation are a lack of owner compliance or loss of contact with owners, as well as overly high expectations of success. Improved education and communication, regular check-ups, and strict adherence to ASIT guidelines can increase the number of dogs that successfully respond to and benefit from ASIT.
Dr. Elisabeth Reinbacher
Range of Services – serological allergy tests
Intracutaneous Allergy Tests
Allergen-Specific Immunotherapy


